# Endocarditis
- Modified Duke Criteria: ***
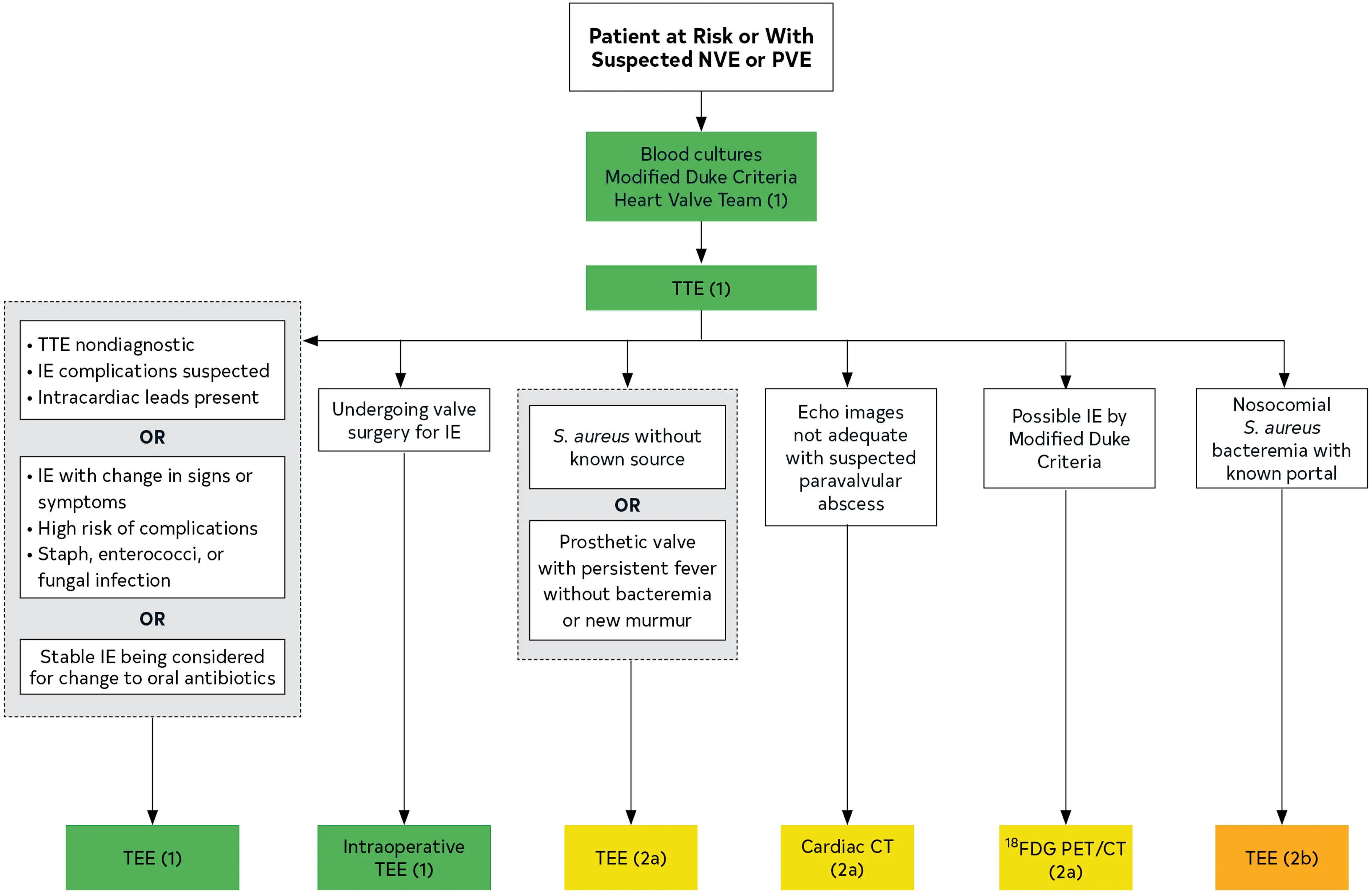
- If possible IE, plan for FGD-PET/CT
- BC x2
- TTE ordered to assess for vegetations, characterize the hemodynamic severity of valvular lesions, assess ventricular function and pulmonary pressures, and detect complications
- If TTE nondiagnostic, plan to proceed with TEE
- If paravalvular infection suspected, will order CT- Valves affected:
- MV > AV > TV > PV
- Microorganisms most commonly involved:
- Staph aureus (31%)
- Strep viridans (17%)
- Post-op: Staph epi early (within 2 months of valve surgery)
- Risk factors for IE:
- Age
- IVDU
- HD/IV lines
- Cancer
- Immunosuppression
- Structural heart disease
- Prosthetic valve/devices
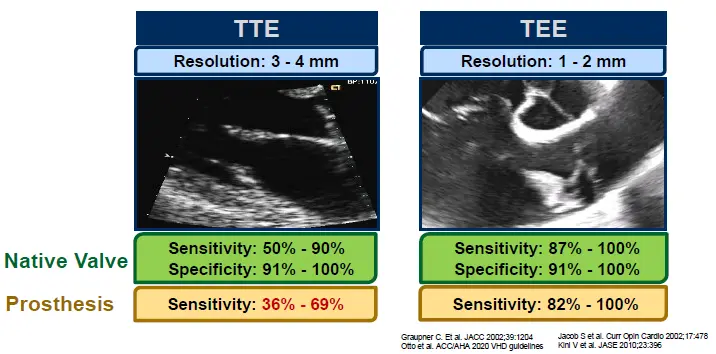
- TEE has better sensitivity for detecting bacterial endocarditis compared to TTE
- Native valve vs. Prosthetic valve? - Timing of infection after valve intervention?
- Fatal if untreated
- in-hospital mortality rate is 15% to 20%, with a 1-year mortality rate approaching 40% 1
Diagnosis
- In a study by Kim et al, the detection rate of vegetations by TEE was superior to CCT (94.4% versus 52.8%) for small vegetations measuring <10 mm.2
- While TEE remains the initial diagnostic tool in patients with suspected PVE, its sensitivity has been reported between 82% and 94% compared with 90% and 100% in native valve IE. Therefore, in cases of benign initial TEE, it is often necessary to observe and repeat the TEE or perform further imaging such as CCT or 18F-FDG PET/CT if the index of suspicion is high or if there is a change in clinical status (persistent fever or positive blood cultures, new neurological symptoms, or signs of distal embolization).2
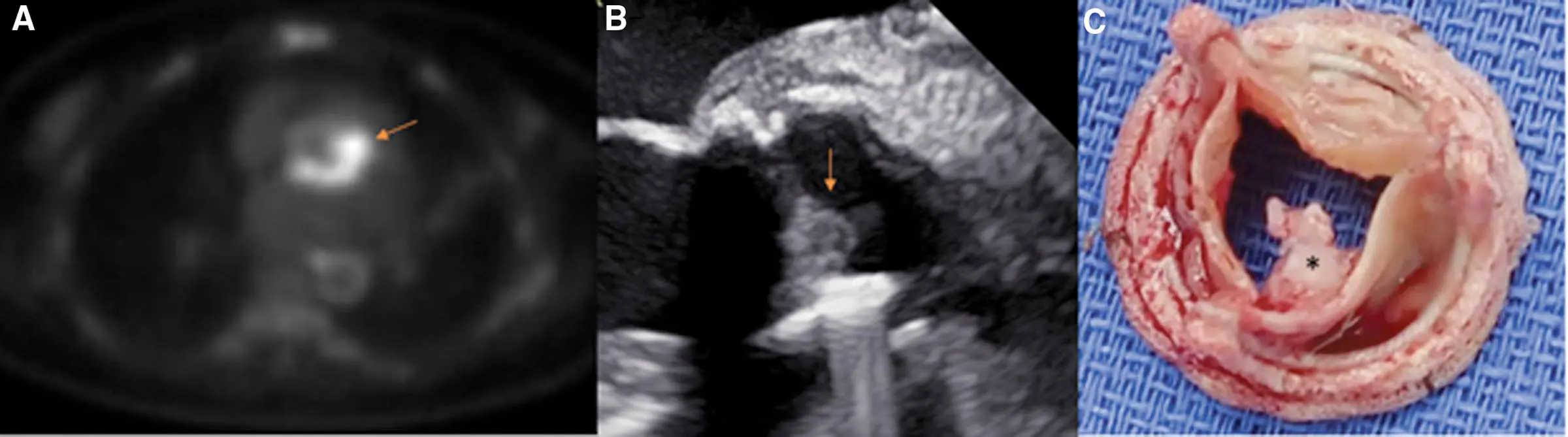
- A 53-year-old female with a history of quadricuspid aortic valve status post-aortic valve replacement (AVR) 3 years before presentation presented with fevers, chills, and speech changes. Computed tomography (CT) of the brain revealed cerebellar infarcts. A transthoracic echocardiogram did not reveal evidence of endocarditis, and thus a transesophageal echocardiogram (TEE) was obtained. TEE did not reveal vegetations, but 18F-fluorodeoxyglucose positron emission tomography/computed tomography showed intense focal fluorodeoxyglucose uptake around the aortic prosthesis concerning prosthetic valve endocarditis with an aortic root abscess (A, arrow). Blood cultures grew methicillin-sensitive Staphylococcus aureus. She was referred for a redo of the AVR. Operative TEE revealed large vegetation attached to the aortic valve bioprosthesis (B, arrow), which was again seen on the explanted valve (C, star).2
- WBC-SPECT has important disadvantages over 18F-FDG PET, including low diagnostic sensitivity, a higher radiation dose, lower image resolution, long acquisition, and the need for complex blood handling.2
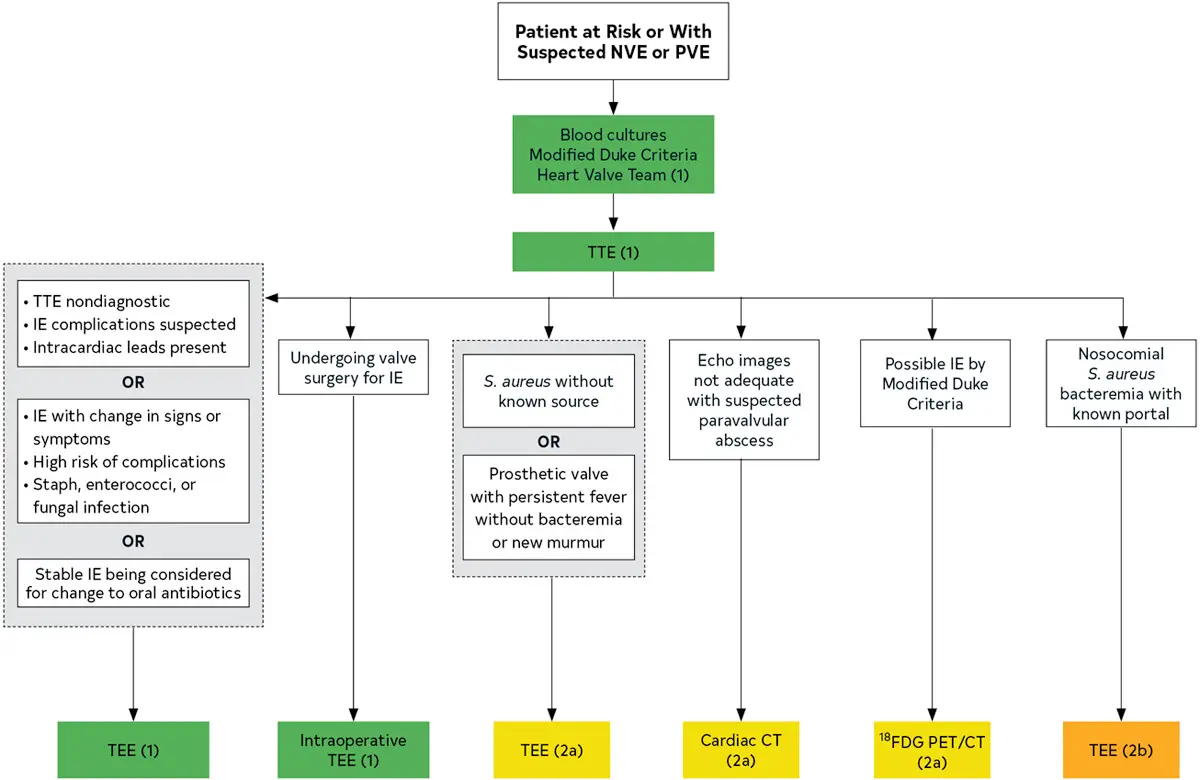 Figure source: 1
Figure source: 1
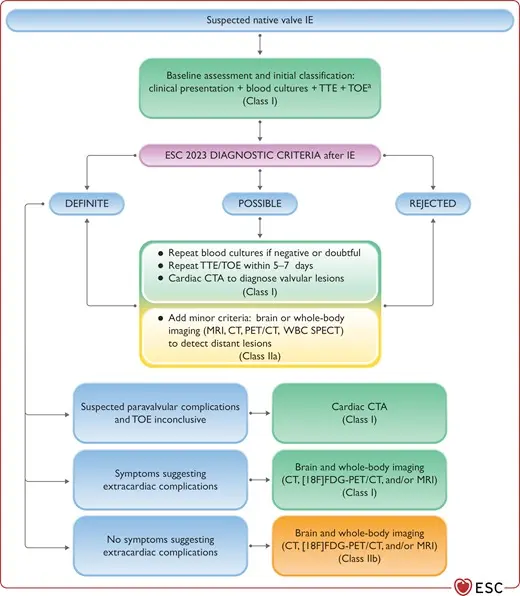
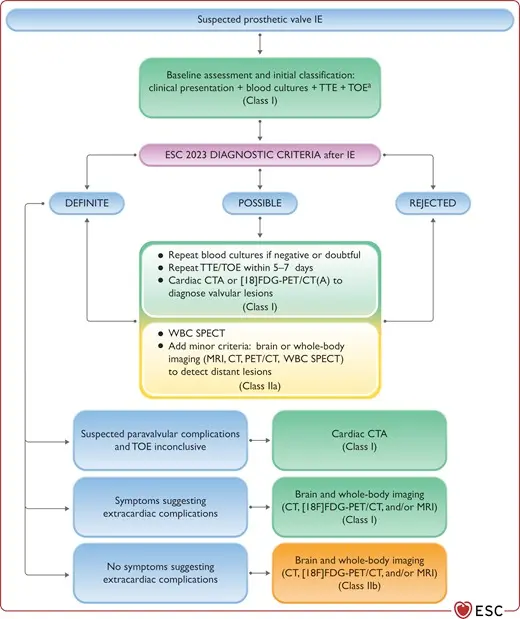
Table source: 2
| Modality | Strength | Limitations |
|---|---|---|
| Echocardiography (TTE/TEE) | • Highest temporal resolution. • Best for evaluation of small vegetations, fistulas, leaflet perforation, and valve dehiscence. • No radiation. • Broad availability. | • Limited sensitivity for perivalvular complications of PVE due to prosthetic material shadowing. • Sedation needed for TEE. |
| Cardiac computed tomography | • Best for evaluation of abscess and pseudoaneurysm. • Fast acquisition. • Suitable for hemodynamically unstable patients. • Provides preoperative evaluation (coronary assessment, proximity of cardiovascular structures to sternum, and aortic calcification). | • Low sensitivity for small vegetations (<10 mm) and perforations. • Radiation exposure. • Need for iodine-based contrast. • Metallic beam-hardening artifact may preclude lead and generator pocket evaluation. • Scan quality dependent on scanner and technologist. |
| 18F-FDG PET/CT | • High sensitivity. • Provide whole-body imaging for evaluation of all intravascular prosthetic materials and distant emboli. • Fast acquisition. | • Nonspecific for infection (limited use in 1–3 mo postsurgery). • Radiation exposure. • Limited availability. • Need for handling radioactive material. |
| Tagged WBC-SPECT | • High specificity (particularly beyond 4 wk after surgery). • No need for dietary preparation. • Can provide whole-body imaging. | • Low sensitivity. • Lower image resolution. • Long procedure (several time point acquisitions). • Need for complex blood handling. • Need for handling radioactive material. |
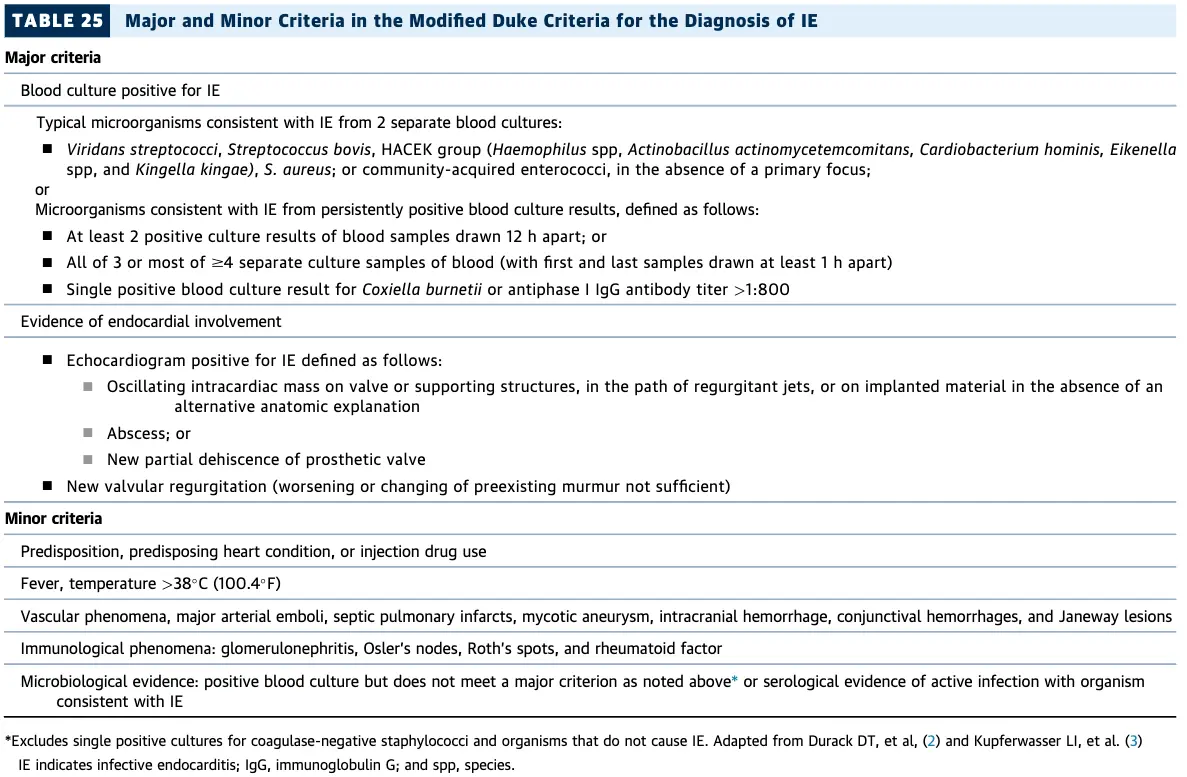
Modified Duke Criteria
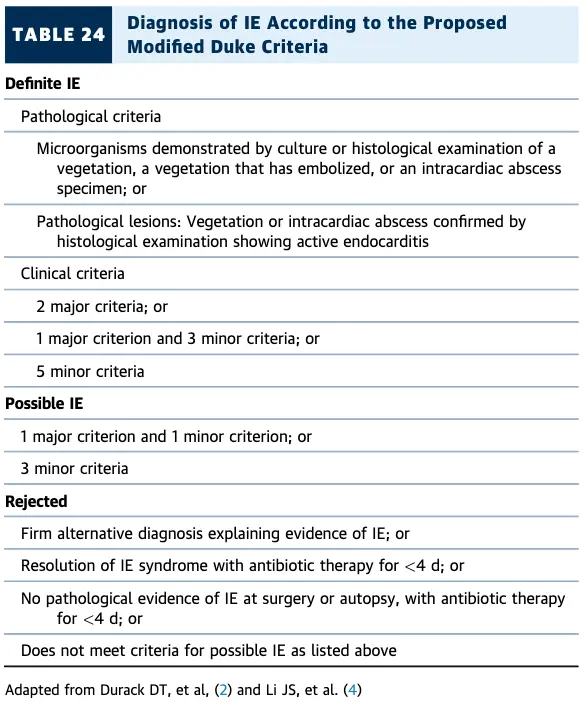
Echo
Prosthetic valve endocarditis (PVE) may have NO vegetation
⚠️ 30-40% cases of prosthetic valve endocarditis (PVE) have NO vegetation attached to the prosthesis, only peri-annular infection. ∴, you may want to consider TEE or other imaging modalities for PVE.
- Echo reports for IE should comment on the following:
- Diagnosis: confirm presence, location, size, number & morphology of the vegetation(s)
- Structural complications
- Local severity of valve destruction
- Impact on surrounding structures abscess, fistula, aneurysm, dehiscence
- Systemic embolization
- Hemodynamic impact
- Acute regurgitation, CHF, shunt, tamponade, valve obstruction, hemolysis
- TTE vs TEE
- TTE can pick up a vegetation as big as 3-4 mm, whereas TEE can pick up a veg as small as 1-2 mm
- Class I indications for TEE?
- Suspected IE +
- non-diagnostic TTE, suspect IE complications, intracardiac leads present OR
- IE with change in Si/Sx, high risk of complications, Infection with Staph/Strep/Enterococci
- Stable IE and considering switch from IV → PO Abx
- Suspected IE +
- DDx for mobile endocardial echodensity:
- Lambl’s excrescence, fenestration
- Vegetation: infective/non-infective (healed)
- e.g. Libman-Sacks endocarditis
- Sclerosis/calcium artifact, MAC
- Ruptured/retracted chordae
- Myxomatous tissue
- Valvular strands, surgical remnants
- Papillary fibroelastoma, myxoma
- Thrombus (e.g. prosthetic thrombosis)
- Characteristics of vegetations (Major criteria of Duke’s for “Evidence of endocardial involvement”)
- Motion:
- oscillating intracardiac mass on valve, supporting structures, or prosthesis; independent motion
- Effects:
- new regurgitation (worsening or changing or pre-existing murmur is not sufficient)
- abscess
- new partial dehiscence of prosthetic valve
- Location:
- Upstream side of the valve in the path of the regurgitant jet or on prosthetic material
- No alternative anatomic explanation
- Texture:
- Gray scale, similar reflectance of myocardium
- Shape:
- Lobulated and amorphous
- Motion:
Cardiac CTA
- With CCT, a vegetation is seen as a hypodense, homogeneous, irregular mass on a valve, endocardial structure or implantable cardiac material. 2
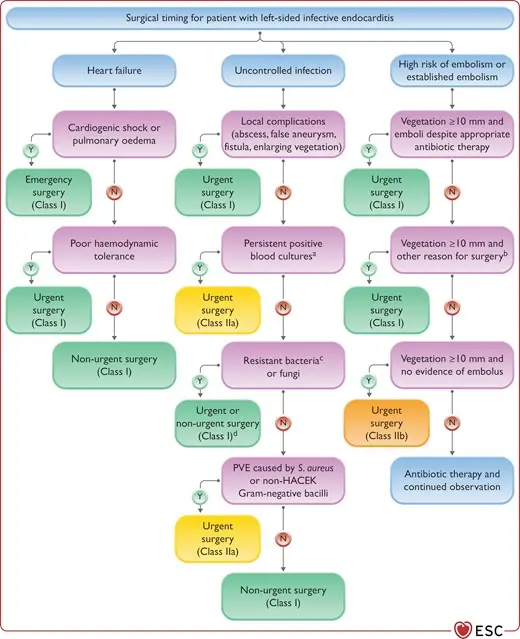
Management
Complications
- Manifestations of prosthetic valve endocarditis include vegetations, abscess, pseudoaneurysm, fistula, leaflet perforation, dehiscence, and abnormal nuclear tracer uptake.2
Abscess
- After vegetations, abscesses represent the second most typical finding of PVE.2
- By echocardiography, an abscess is identified as a thickened, irregular, and inhomogeneous area or mass with an echodense or echolucent appearance.2
- With CCT, an abscess is defined as a perivalvular collection of liquid density or a thick layer of inflammatory tissue that enhances contrast media.2
Pseudoaneurysm
- Pseudoaneurysms are pulsatile perivalvular cavities with evidence of color Doppler flow or contrast enhancement that is simultaneous with the cardiac or aortic lumen. A pseudoaneurysm results as a complication of an abscess when it erodes or ruptures toward the intracardiac or aortic lumen.2
Intracardiac fistula
- Progression to involve the valve annulus → fistula between the LA and LV, which could result in significant regurgitation.
- An intracardiac fistula is a pathological communication between 2 neighboring cavities through perforation or erosion. It can be identified using color Doppler (transthoracic echocardiogram and TEE) or by direct visualization of a fistulous tract with echocardiography and CCT. In CCT, a fistula appears as a contrast-filled tract that connects 2 neighboring cavities.2
- TEE is more effective than CCT in accurately identifying intracardiac fistula due to its better temporal resolution.2
Leaflet perforation
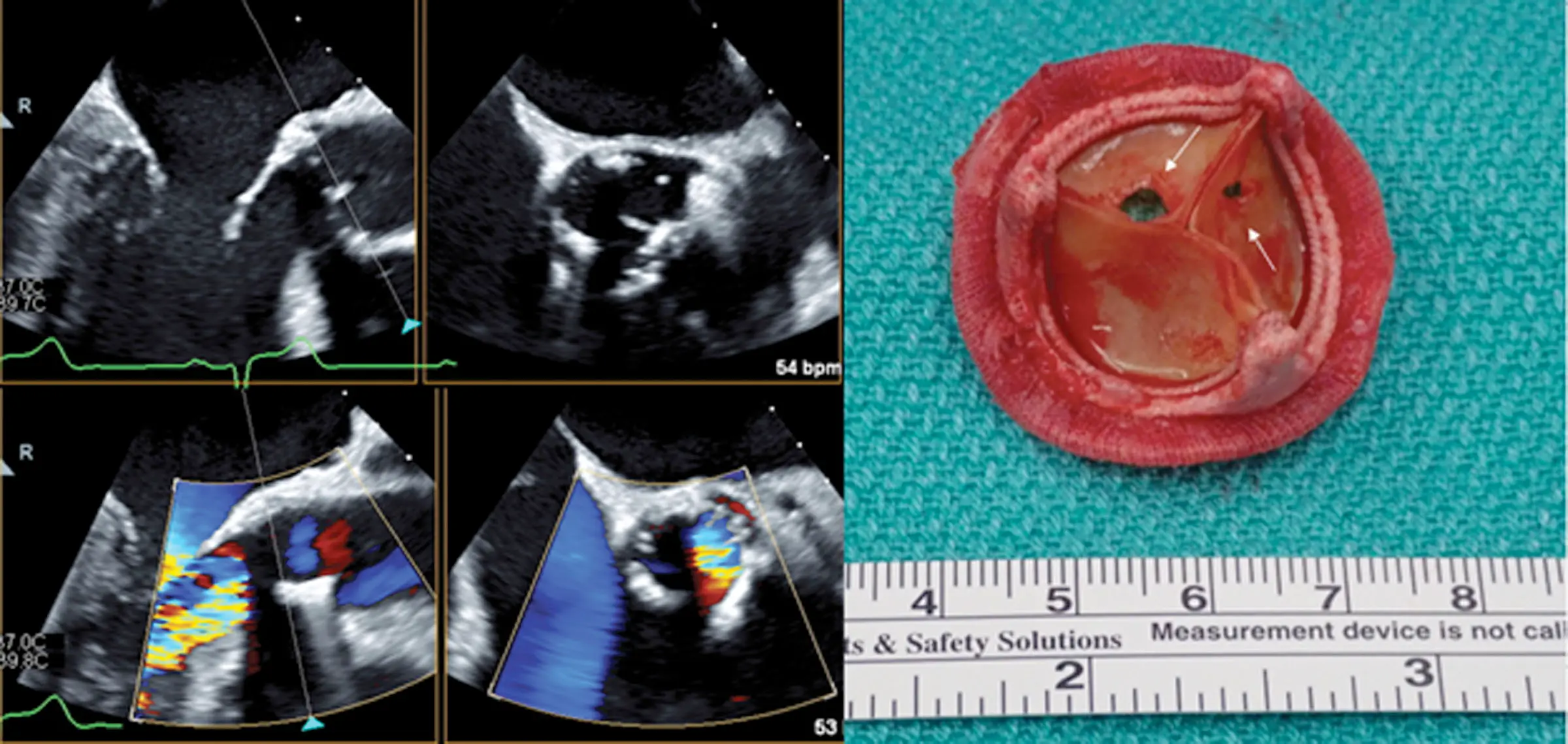 Figure source: 2
Figure source: 2
Valvular Dehiscence
 (A) Transesophageal echocardiography, mid-esophageal long-axis view, demonstrates a prominent aortic root abscess cavity (white arrow) posteriorly in a patient with a prosthetic aortic valve. Also note partial dehiscence of the aortic bioprosthesis (red arrow). (B) Color Doppler analysis demonstrates significant aortic regurgitation between the aortic bioprosthesis and the left ventricular outflow tract through the prominent abscess cavity. (Source)
(A) Transesophageal echocardiography, mid-esophageal long-axis view, demonstrates a prominent aortic root abscess cavity (white arrow) posteriorly in a patient with a prosthetic aortic valve. Also note partial dehiscence of the aortic bioprosthesis (red arrow). (B) Color Doppler analysis demonstrates significant aortic regurgitation between the aortic bioprosthesis and the left ventricular outflow tract through the prominent abscess cavity. (Source)
Footnotes
-
Otto, C. M., Nishimura, R. A., Bonow, R. O., Carabello, B. A., Erwin, J. P., Gentile, F., Jneid, H., Krieger, E. V., Mack, M., McLeod, C., O’Gara, P. T., Rigolin, V. H., Sundt, T. M., Thompson, A., & Toly, C. (2021). 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Journal of the American College of Cardiology, 77(4), e25–e197. https://doi.org/10.1016/j.jacc.2020.11.018 ↩ ↩2
-
Hutt E, Canosa FJM, Unai S, Jaber WA. Manifestations of Prosthetic Valve Endocarditis: Lessons From Multimodality Imaging and Pathological Correlation. Circ Cardiovasc Imaging. 2024 Apr;17(4):e016435. doi: 10.1161/CIRCIMAGING.123.016435. Epub 2024 Apr 16. PMID: 38626096. ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7 ↩8 ↩9 ↩10 ↩11 ↩12 ↩13 ↩14