- Pulmonary hypertension (PH) is now defined by a mean pulmonary arterial pressure >20 mmHg at rest. The definition of Pulmonary Arterial Hypertension (PAH) also implies a pulmonary vascular resistance (PVR) >2 Wood Units and pulmonary arterial wedge pressure ≤15 mm Hg.1
- “Recent data from normal subjects has shown that normal mPAP was 14.0±3.3 mmHg. Two standard deviations above this mean value would suggest mPAP >20 mmHg as above the upper limit of normal (above the 97.5th percentile). This definition is no longer arbitrary, but based on a scientific approach.” (Source)
- It is essential to include PVR and pulmonary arterial wedge pressure (PAWP) in the definition of pre-capillary PH, in order to discriminate elevated PAP due to pulmonary vascular disease (PVD) from that due to left heart disease (LHD), elevated pulmonary blood flow, or increased intrathoracic pressure.2
- Classified into 5 groups based on etiology of PH as defined by the 2018 World Symposium on Pulmonary Hypertension (WSPH)
- Group 1, or PAH, also requires normal left heart filling pressures (PCWP or LVEDP ≤ 15 mmHg) with PVR ≥ 2 WU.
- Group 3 (PH due to lung disease, hypoxia or both), Group 4 (PH due to pulmonary artery obstructions), and Group 5 (PH with multifactorial or unclear mechanisms) share similar hemodynamic criteria to Group 1 PH.
- Group 2 (PH due to left heart disease) is diagnosed when PCWP > 15mmHg at rest or may be suggestive with significant increases in PAWP during provocative maneuvers during RHC (e.g. saline infusion or exercise).
| Definition | Hemodynamic characteristics |
|---|---|
| PH | mPAP >20 mmHg |
| Pre-capillary PH | mPAP >20 mmHg PAWP ≤15 mmHg PVR >2 WU |
| IpcPH | mPAP >20 mmHg PAWP >15 mmHg PVR ≤2 WU |
| CpcPH | mPAP >20 mmHg PAWP >15 mmHg PVR >2 WU |
| Exercise PH | mPAP/CO slope between rest and exercise >3 mmHg/L/min |
| PCWP ≤15 mmHg | PCWP >15 mmHg | |
|---|---|---|
| PVR ≤ 2 WU | Consider high-flow state | Isolated post-capillary PH (IpcPH) |
| PVR > 2 WU | Pre-capillary PH | Combined post-capillary PH (CpcPH) |
-
Pre-capillary PH
- Pre-capillary PH is best defined by the concomitant presence of mPAP >20 mmHg, PAWP ≤15 mmHg and PVR ≥3 WU, emphasizing the need for RHC with mandatory measurement of CO and accurate measurement of PAWP.2
- PVR ≥3 WU:
- Including PVR (recall, ) in the definition of pre-capillary PH is essential, allowing discrimination of elevation of PAP due to PVD from those due to elevation of PAWP or due to high CO.2
-
Post-capillary PH
- Post-capillary PH is hemodynamically defined as mPAP >20 mmHg and PCWP >15 mmHg.
- PVR is used to differentiate between patients with post-capillary PH who have a significant pre-capillary component:
- PVR >2 WU: combined post- and pre-capillary PH (CpcPH)
- PVR ≤2 WU: isolated post-capillary PH (IpcPH)
-
Elevated mPAP (>20 mmHg) but low PVR (≤2 WU) and low PAWP (≤15 mmHg) is categorized by elevated pulmonary blood flow (may be described by the term ‘unclassified PH’ and, although they have PH, they do not fulfil the criteria of pre- or post-capillary PH.2
- Patients with unclassified PH may present with congenital heart disease (CHD), liver disease, airway disease, lung disease, or hyperthyroidism explaining their mPAP elevation.
- Clinical follow-up of these patients is generally recommended. In the case of elevated pulmonary blood flow, its etiology should be explored.
-
Despite limited evidence, calcium channel blockers, phosphodiesterase 5 (PDE5) inhibitors, and inhaled/IV/subcutaneous prostacyclin analogues are considered safe during pregnancy 🤰.1
-
Now, there is a recommendation for PH medical therapy in group 3 PH, based on a single positive randomized controlled trial in patients with interstitial lung disease (ILD). The therapeutic approach to group 3 PH starts with optimizing the treatment of the underlying lung disease, including supplementary oxygen and noninvasive ventilation, where indicated, as well as enrollment into pulmonary rehabilitation programs. The new recommendation is that PDE5 inhibitors may be considered in patients with severe PH associated with ILD with individual decision-making in PH centers.1
-
In the present clinical classification of PH, pre-capillary PH concerns patients from groups 1, 3 and 4, some patients from group 5, and rarely patients from group 2 with combined pre- and post-capillary PH.
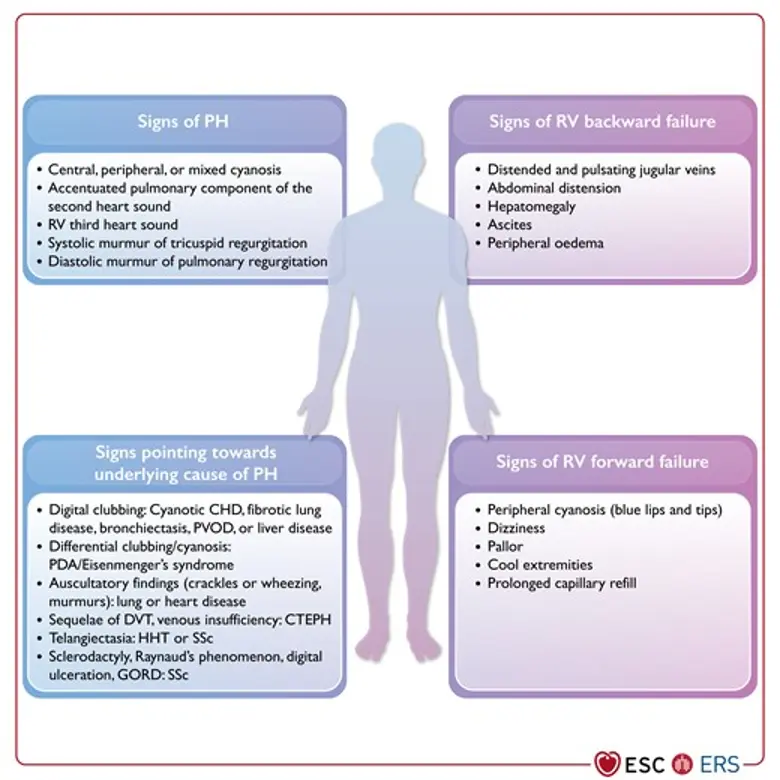
Exam Findings
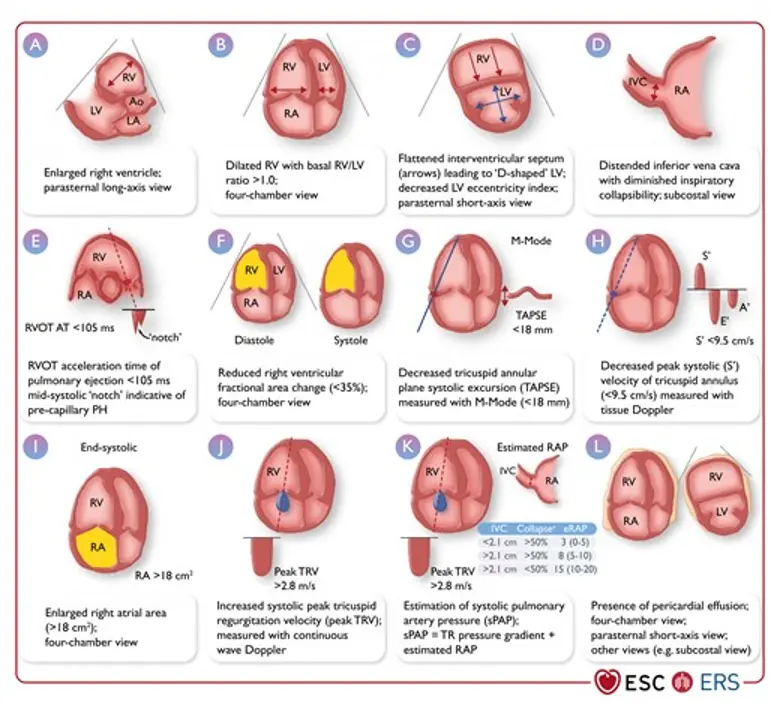
Echo Findings
- PV acceleration time < 105 ms is highly suggestive of pulmonary hypertension
Additional echocardiographic signs suggestive of pulmonary hypertension2
| A: The ventricles | B: Pulmonary artery | C: Inferior vena cava and RA |
|---|---|---|
| RV/LV basal diameter/area ratio >1.0 | RVOT AT <105 ms and/or mid-systolic notching | IVC diameter >21 mm with decreased inspiratory collapse (<50% with a sniff or <20% with quiet inspiration) |
| Flattening of the interventricular septum (LVEI >1.1 in systole and/or diastole) | Early diastolic pulmonary regurgitation velocity >2.2 m/s | RA area (end-systole) >18 cm2 |
| TAPSE/sPAP ratio <0.55 mm/mmHg | PA diameter >AR diameter PA diameter >25 mm |
Systolic Septal Flattening
The following are examples of systolic septal flattening, which can occur in the context of RV pressure overload.
Vasoreactivity Testing
- The purpose of vasoreactivity testing in PAH is to identify acute vasoresponders who may be candidates for treatment with high-dose CCBs.
- Pulmonary vasoreactivity testing is only recommended in patients with IPAH, HPAH, or DPAH.
- A positive acute response is defined as a reduction in mPAP by ≥10 mmHg to reach an absolute value ≤40 mmHg, with increased or unchanged CO.
Footnotes
-
https://www.acc.org/Latest-in-Cardiology/ten-points-to-remember/2022/08/30/19/11/2022-ESC-Guidelines-for-Pulmonary-Hypertension-ESC-2022 ↩ ↩2 ↩3
-
Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, Ferreira DS, Ghofrani HA, Giannakoulas G, Kiely DG, Mayer E, Meszaros G, Nagavci B, Olsson KM, Pepke-Zaba J, Quint JK, Rådegran G, Simonneau G, Sitbon O, Tonia T, Toshner M, Vachiery JL, Vonk Noordegraaf A, Delcroix M, Rosenkranz S; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022 Oct 11;43(38):3618-3731. doi: 10.1093/eurheartj/ehac237. Erratum in: Eur Heart J. 2023 Apr 17;44(15):1312. doi: 10.1093/eurheartj/ehad005. PMID: 36017548. ↩ ↩2 ↩3 ↩4 ↩5