- Normal (e.g. LVEF, wall thickness, etc.), but with restrictive filling patterns
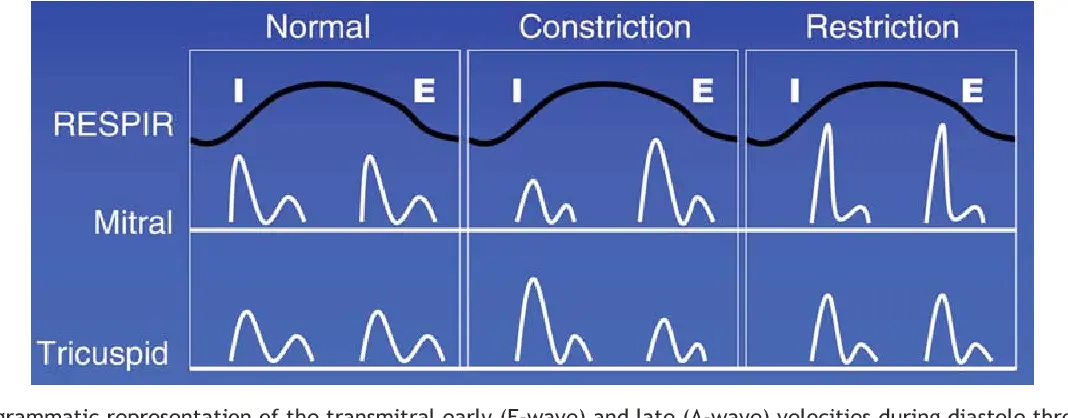
- 📝 Many disorders manifest restrictive “physiology” and must be excluded (eg, Hypertrophic Cardiomyopathy and Constrictive Pericarditis)
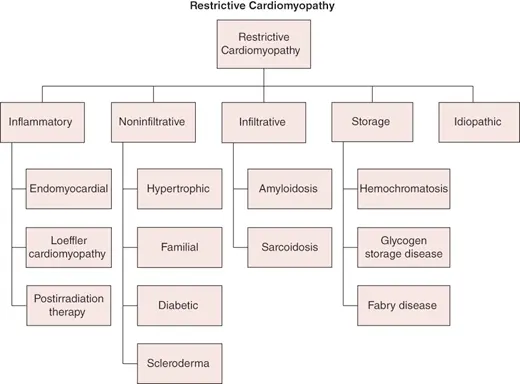
Classification
| Cardiac Involvement | Type | Pathology |
|---|---|---|
| Myocardial | Non-infiltrative | Idiopathic Familial Scleroderma |
| Myocardial | Infiltrative | Amyloidosis Fabry’s Disease |
| Myocardial | Storage Disease | Gaucher’s |
| Endomyocardial | N/A | Endomyocardial fibrosis Hypereosinophilia Carcinoid heart disease Metastatic cancer Radiation Anthracycline toxicity Drugs (ergotamine) Prior cardiac operation |
- Echo
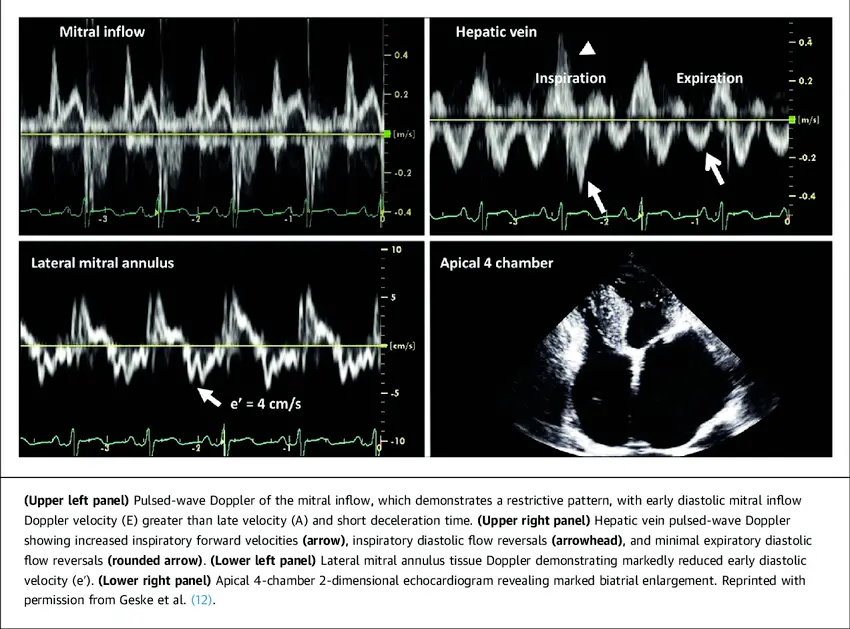
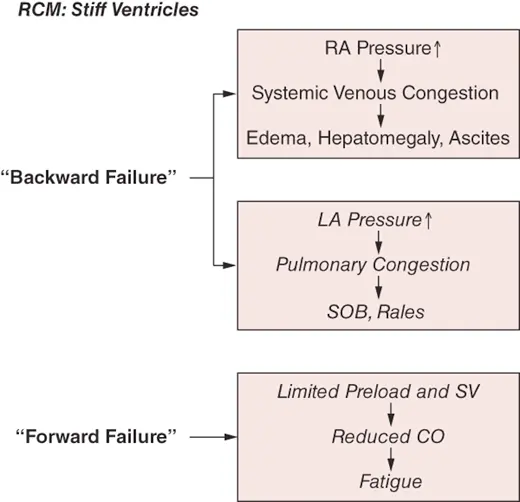
- Atrial enlargement
- reflects ventricular noncompliance and may also result from primary atrial myocardial involvement by the disease process (eg, amyloidosis)
- Doppler
- Rapid E wave with short deceleration time (indicating ↑ early LV filling velocity) and very little atrial contribution to ventricular filling (i.e. relatively small A-wave)
- ↓ isovolumic relaxation time
- Pulmonary vein doppler: almost no systolic forward flow and mostly all forward flow is seen in early diastole
- Tissue Doppler velocity shows a very low e’ velocity
- Restrictive filling can be easily recognized by an increased E/A ratio (>2) along with a very short deceleration time of the E wave (<160 ms). In this situation, the LA is enlarged, and e′ is reduced (< 5 cm/s).1
- Rapid E wave with short deceleration time (indicating ↑ early LV filling velocity) and very little atrial contribution to ventricular filling (i.e. relatively small A-wave)
- Cath Hemodynamics
- ↑ Filling Pressures
- Dip and plateau morphology (aka “square-root sign”)
- nonspecific indicator of stiff noncompliant chambers
- LVEDP >5 mm Hg + RVEDP
- RVEDP <1/3 of RVSP
- RVSP >50 mmHg
- Ventricular concordance
Management
- Idiopathic RCM
- Cautious Diuresis
- Many patients are dependent on preload, ∴ can’t lower it too much otherwise patients will have a ↓ in BP and feel like 💩
- Beta-blockers, but not as aggressive as DCM
- Filling in RCM is restricted to early diastole, ∴ if you ↓ HR down too much → restrict overall cardiac output
- Cardiac Transplantation (esp if advanced)
- Cautious Diuresis
Footnotes
-
Oh JK, Park SJ, Nagueh SF. Established and novel clinical applications of diastolic function assessment by echocardiography. Circ Cardiovasc Imaging. 2011 Jul;4(4):444-55. doi: 10.1161/CIRCIMAGING.110.961623. PMID: 21772012. ↩