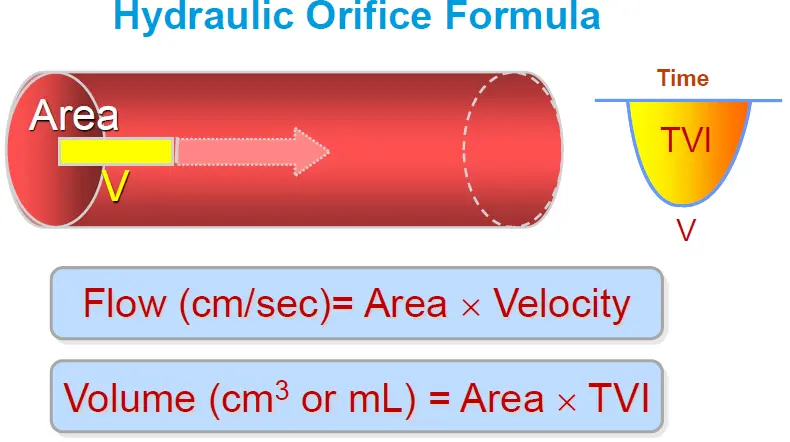
Hydraulic Orifice Formula
Stroke Volume
Thus,
Echo-Based Qp/Qs (Intracardiac Shunts)
Cardiac Output
Cardiac Index
def calculate_hemodynamics(vti_lvot, lvot_diameter, heart_rate, bsa,
sbp, dbp, est_rap):
stroke_volume = 0.785 * (lvot_diameter ** 2) * vti_lvot
svi = (stroke_volume / bsa) if bsa != 0 else 0
cardiac_output = stroke_volume * heart_rate
cardiac_index = cardiac_output / bsa
map = (sbp + (2 * dbp)) / 3
svr = (map - est_rap) / cardiac_output
return stroke_volume, svi, cardiac_output, cardiac_index, svrContinuity Equation for Aortic Valve Area
- Echo Measurements (ASE guidelines)
- View: PLAX, zoomed up view
- Inner-edge to inner-edge in mid-systole
- Make measurements parallel and adjacent to the aortic valve or at the site of velocity measurement within 5 mm of the aortic annulus (where you’ll likely be assessing LVOT VTI)
- Aortic valve VTI is obtained using CWD
Continuity Equation is based on the preservation of flow. In other words, the flow through the aortic valve will be equal to the flow through the LVOT. This translates into .
Consider fluid moving through a tube: the flow at point is the same as point if the size at each of the two points is the same. But, if the diameter of the tube at is 1/2 that of , then the flow at will be double that at .
From the Mayo Board Review course, which highlights the importance of assessing for the AV VTI from multiple windows‼️
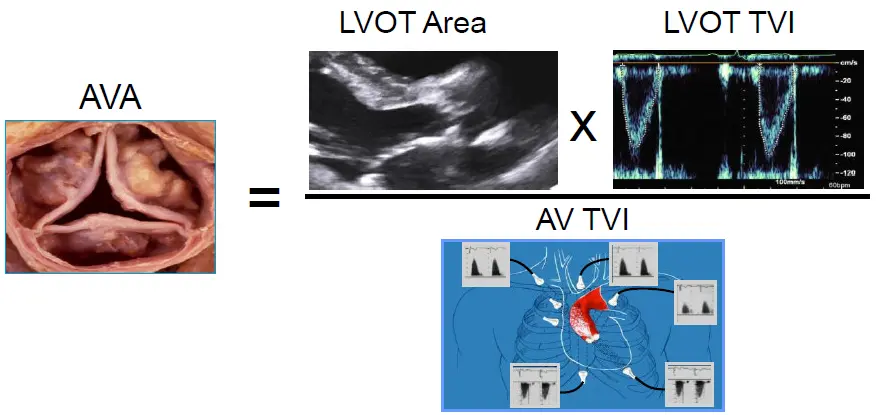
def calculate_aortic_stenosis(vmax, vti_lvot, vti_ao, lvot_diameter):
mean_gradient = 4 * (vmax ** 2)
stroke_volume = 0.785 * (lvot_diameter ** 2) * vti_lvot
ava = (stroke_volume / vti_ao) if vti_ao != 0 else 0
return mean_gradient, stroke_volume, avaSystemic Vascular Resistance (SVR)
Using IVC collapsibility indices to estimate RAP, and arm blood pressure measurements to calculate mean arterial pressure, SVR (in Wood units) can be calculated as
Pulmonary Vascular Resistance (PVR)
Using Echo hemodynamics, you may also be able to calculate PVR with the following equation:
where TR is measured in m/s and RVOT VTI in cm
Pressure Half Time (PHT)
Mitral Valve Area (MVA) from PHT
Modified Bernoulli Equation for Pressure Gradients
These often involve measuring a pressure gradient across a “leaky” structure (e.g. TR, VSD, PFO, PDA, etc.), where we are measuring the maximal gradient between two different pressures of the heart that are separated by the “leaky” structure. For example, in the case of TR, we are measuring the gradient between the RA and RV. Importantly, maximal regurgitation gradient isn’t all that helpful WITHOUT a reference point, and in Echo these often will be RAP, SBP, DBP.
| Structure | Gradient Between |
|---|---|
| Tricuspid Valve | RA + RV |
| Pulmonic Valve | RV + PA |
| Mitral Valve | LA + LV |
| Aortic Valve | LV + Aorta |
| VSD | LV + RV |
| PFO | LA + RA |
RV Systolic Pressure (RVSP)
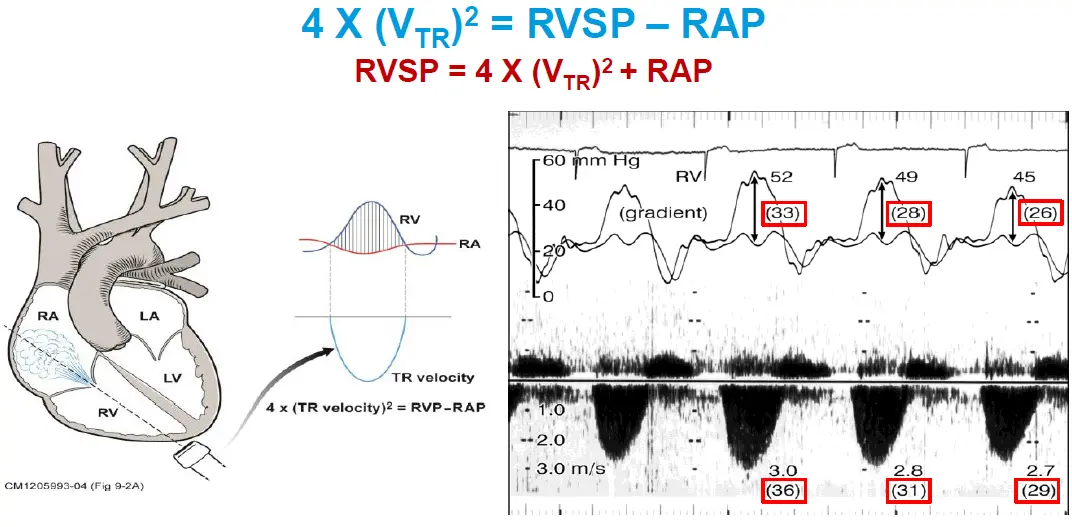
In the case of Ventricular Septal Defect (VSD), the RVSP can be calculated using the following formula:
For example, patient with late-presenting STEMI and found to have VSR. BP was 114/74 mmHg and VSD Doppler tracing below. What is their RVSP? .
LV End-Diastolic Pressure (LVEDP)
📝 We use DBP as a proxy for aorta diastolic pressure.
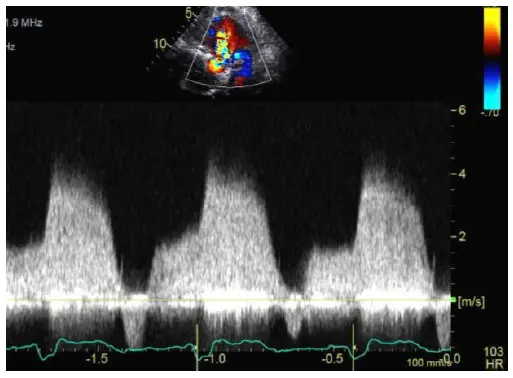
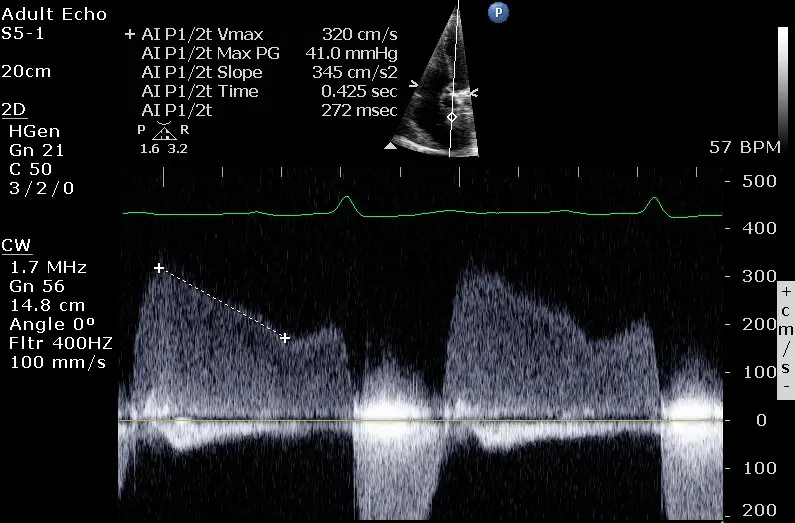 In the above Doppler tracing, is 2 m/s. This example also illustrates the ‘a-dip’ that can sometimes be seen with Aortic Regurgitation.
In the above Doppler tracing, is 2 m/s. This example also illustrates the ‘a-dip’ that can sometimes be seen with Aortic Regurgitation.
PA End-Diastolic Pressure (PAEDP)
📝 Technically, you’ll want to use RVEDP in place of RAP. However, physiologically RAP = RVEDP, so it should work to use RAP instead.
Left Atrial Pressure (LAP)
📝 We can’t easily measure , so we use SBP as a surrogate 👆as the two values should be similar.
For example, a patient with peak mitral valve gradient of 3 m/s and BP of 100/54. The LAP would be mmHg!
In the setting of a PFO, the LAP can be estimated using the following formula:
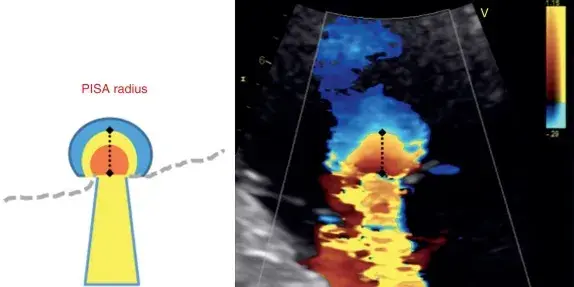
Proximal Isovelocity Surface Area (PISA)
- Exploits Doppler color flow aliasing.
- As fluid in a container goes through a narrow orifice, the velocity ↑. With PISA, we take advantage of this phenomenon by shifting our Doppler baseline in the direction of flow. This exposes these “hemispheres” that correspond to different velocities that we can use to calculate regurgitant/stenotic flow.
- The flow at the PISA should be equal to the flow at the narrowest portion, which is termed the effective regurgitant orifice (ERO); the area of which is referred to as the ERO area (or EROA)
PISA for Regurgitation
Direction of PISA radius measurement
You will draw the line for PISA radius calculation towards the direction of the ultrasound beam