Echo
Reference Ranges
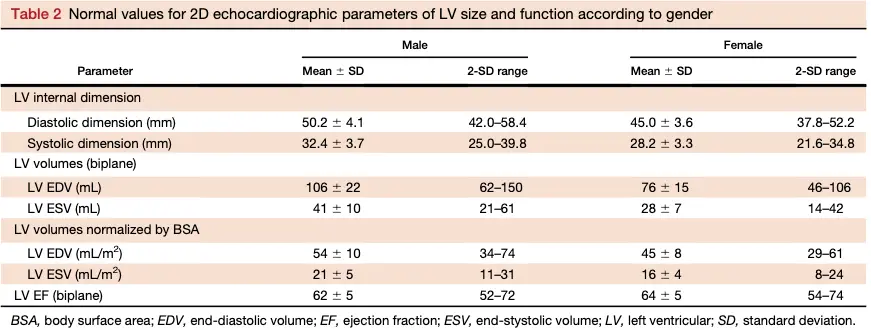
LV size
- For general reference, 2D echocardiographic LVEDVs of 74 mL/m^2 for men and 61 mL/m^2 for women and LVESVs of 31 mL/m^2 for men and 24 mL/m^2 for women should be used as the upper limits of the corresponding normal range.
| LVEDV (mL/m^2) | LVESV (mL/m^2) | |
|---|---|---|
| Men | 74 | 31 |
| Women | 61 | 24 |
 |
LVEF & LA volume

Table 4 Normal ranges and severity partition cutoff values for 2DE-derived LV EF and LA volume
| Male | Male | Male | Male | Female | Female | Female | Female | |
|---|---|---|---|---|---|---|---|---|
| Normal range | Mildly abnormal | Moderately abnormal | Severely abnormal | Normal range | Mildly abnormal | Moderately abnormal | Severely abnormal | |
| LV EF (%) | 52-72 | 41-51 | 30-40 | <30 | 54-74 | 41-53 | 30-40 | <30 |
| Maximum LA volume/BSA (mL/m) | 16-34 | 35-41 | 42-48 | >48 | 16-34 | 35-41 | 42-48 | >48 |
Left atrial volume cutoffs
You know the ULN is 34. Add 7 to get the cutoff for mild (41), another 7 for moderate (48), beyond which it is considered ‘severe.‘
LV Mass
Use the following formula to calculate relative wall thickness (RWT):
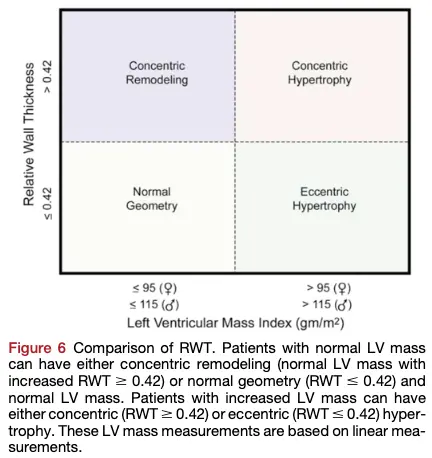
Table 6 Normal ranges for LV mass indices
| Women | Men | |
|---|---|---|
| Linear method | ||
| LV mass (g) | 67-162 | 88-224 |
| LV mass/BSA (g/m) | 43-95 | 49-115 |
| Relative wall thickness (cm) | 0.22-0.42 | 0.24-0.42 |
| Septal thickness (cm) | 0.6-0.9 | 0.6-1.0 |
| Posterior wall thickness (cm) | 0.6-0.9 | 0.6-1.0 |
| 2D method | ||
| LV mass (g) | 66-150 | 96-200 |
| LV mass/BSA (g/m) | 44-88 | 50-102 |
Measuring LV Systolic Function
Recall, so we will estimate LV global systolic function by measuring the difference between the end-diastolic and end-systolic value.
- The biplane method of disks (modified Simpson’s rule) is the currently recommended 2D method to assess LVEF by the ASE Writing Committee.
- When to measure?
- End-diastole is preferably defined as the first frame after mitral valve closure or the frame in the cardiac cycle in which the respective LV dimension or volume measurement is the largest.
- End-systole is best defined as the frame after aortic valve closure or the frame in which the cardiac dimension or volume is smallest.
Measuring LV size
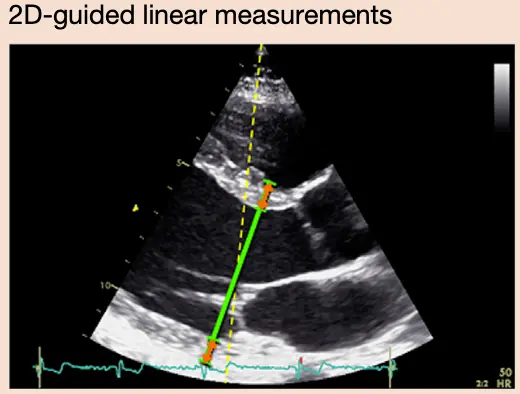
Linear Measurements
- Linear internal measurements of the left ventricle and its walls be performed in the parasternal long-axis view.
- Values should be carefully obtained perpendicular to the LV long axis and measured at or immediately below the level of the mitral valve leaflet tips.
- You want to be perpendicular to the LV long axis, i.e. in line with the flow of blood
Volumetric Measurements
- 3D volumetric measurement
- 🌟 “In patients with good image quality, 3D echocardiographic measurements are accurate and reproducible and should therefore be used when available and feasible.”
- Usually based on tracings of the interface between the compacted myocardium and the LV cavity in the A4C and A2C view
- Contrast agents, e.g. Definity, should be used when needed to improve endocardial delineation when two or more contiguous LV endocardial segments are poorly visualized in apical views, as per published guidelines.
- 📝 Contrast-enhanced images may provide larger volumes than unenhanced images that are closer to those obtained with Cardiac MRI in head-to-head comparison.
- ∴ as a quality check, make sure that the tracings line up well otherwise your measurements will be invalid.
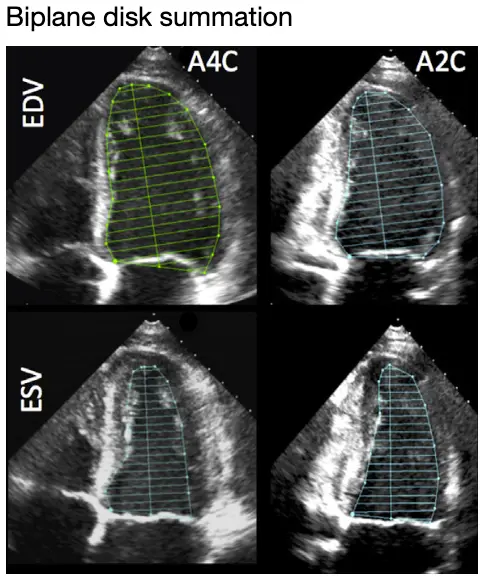
- 🌟 Biplane Method of Disks (MOD) summation (modified Simpson’s rule)
- recommended 2D echocardiographic method by the 2015 Chamber Quantification Guidelines committee
- “At the mitral valve level, the contour is closed by connecting the two opposite sections of the mitral ring with a straight line. LV length is defined as the distance between the middle of this line and the most distant point of the LV contour.” (2015 Guidelines)
- Tip: A4C and A2C lengths should be within 10% of each other, otherwise suggests foreshortening
- ⚠️ make sure you are avoiding papillary muscles, false chords, etc. when doing tracing
- Area-length method
- useful when apical endocardial definition precludes accurate tracing
- the LV is assumed to be bullet shaped, which doesn’t always hold
- Less recommended/Not recommended
- “Volume calculations derived from linear measurements may be inaccurate, because they rely on the assumption of a fixed geometric LV shape such as a prolate ellipsoid, which does not apply in a variety of cardiac pathologies. Accordingly, the Teichholz and Quinones methods for calculating LV volumes from LV linear dimensions are no longer recommended for clinical use.”
Measuring LV Mass
- All measurements should be performed at the end of diastole (the frame before mitral valve closure or the frame in the cardiac cycle in which the ventricular dimension or volume is largest).
- All methods calculate LV volume and then convert the volume to mass by multiplying the volume of myocardium by the myocardial density (approximately 1.05 g/mL).
Cube formula:
Wall Motion Abnormalities
- See the 17-Segment Model
- Not all wma are CAD
- Examples include myocarditis, sarcoidosis, and stress-induced (Takotsubo) cardiomyopathy.
- Abnormal motion patterns of the interventricular septum may be found post-operatively or in the presence of a left bundle branch block or RV epicardial pacing, as well as RV dysfunction caused by RV pressure or volume overload.
- Characteristic motion patterns, which result from abnormal activation sequences, such as septal bounce (“beaking,” “flash”) or lateral apical motion during systole (“apical rocking”) should be reported.