- Gadolinium is not visualized on MRI, but instead facilitates, the relaxation of hydrogen, protons in water
- Is itself toxic, but because it is bound to a specific chelating agent it is safe for use
- When acute infarct/inflammation,
- Rupture of cellular membrane.
- Cellular swelling and edema.
- Gadolinium enters the extracellular space and clears slowly.
- Gadolinium loves collagen and globs onto it
- Gadolinium-based contrast agents (GBCAs) shorten the T1 relaxation time of the surrounding tissues proportional to the local gadolinium concentration. In normal state, gadolinium, which is a large, high-density element made metabolically inert by chelation, enters the extracellular space readily after intravascular injection, but it is unable to cross the cell membrane of a normal myocyte. However, when the myocyte cell membrane is damaged (eg, acute MI) or if there is an increase in the extracellular space between myocytes (eg, acute interstitial edema or chronic fibrosis or MI), GBCA accumulates in the extracellular space, and its washout is delayed after the injection.

- Thus, areas of abnormal myocardium (eg, infarcted, fibrotic, inflamed, or infiltrated myocardium) will have elevated per-voxel GBCA concentration and therefore will have a bright signal on T1-weighted images relative to the surrounding normal myocardium.
- Pattern of delayed enhancement (LGE) suggests diff Dx
- location and appearance (e.g. patchy)
Late Gadolinium Enhancement
- LGE is not disease specific and can be caused by ischemic and non-ischemic necrosis/fibrosis, inflammatory or infectious pathology or tumorous lesions.1
- Most current gadolinium-based contrast agents are extracellular and extravascular. In other words, they do not enter intact myocytes, rather they accumulate within the increased extracellular space or into ruptured myocytes.1
| Coronary pattern | Non-coronary pattern |
|---|---|
| Extends from subendocardium to subepicardium (ischemic wave front) with increasing coronary occlusion time | Subendocardium spared |
| Circumferential extent related to size of perfusion bed and occluded coronary artery | Often more patchy distribution, localized in mid-wall and subepicardium |
| Acute reperfused MI can be associated with MVO | Global subendocardial LGE (uncommon even with diffuse CAD) |
Coronary Pattern
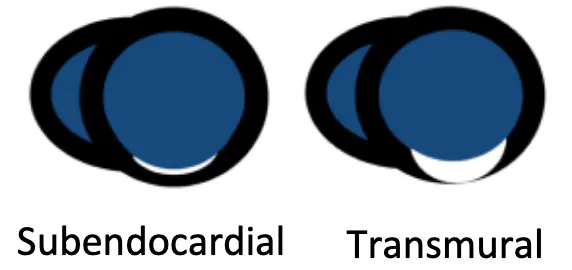
- Subendocardial infarct
- LGE transmurality correlates with likelihood of recovery after revascularization
- LGE identifies arrhythmogenic substrate (mapping for ablation)
- Transmural myocardial infarct
- Degree of transmurality correlates inversely with viability
- Ischaemic cardiomyopathy
- Often also LV dilatation, differential diagnosis of DCM
- Coronary LGE pattern with subendocardial/transmural LGE
- LGE identifies arrhythmogenic substrate (mapping for ablation)
Examples
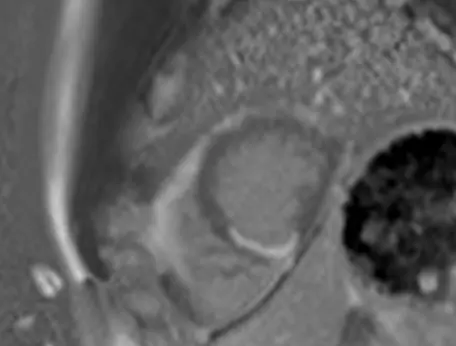
Subendocardial infarct
LGE visualized on PSIR (SAX view with motion correction) reported as “Moderate size area of subendocardial late gadolinium enhancement in the inferior wall consistent with prior presumptive diagnosis of SCAD in the PDA.”
Non-Coronary Pattern
- Cardiac amyloidosis
- Dilated Cardiomyopathy
- Hypertrophic Cardiomyopathy
- Systemic Sclerosis
- Myocarditis
- Fabry’s Disease
- Sarcoidosis
- Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
- Endomyocardial fibrosis (Loeffler’s endocarditis)
- False positive LGE