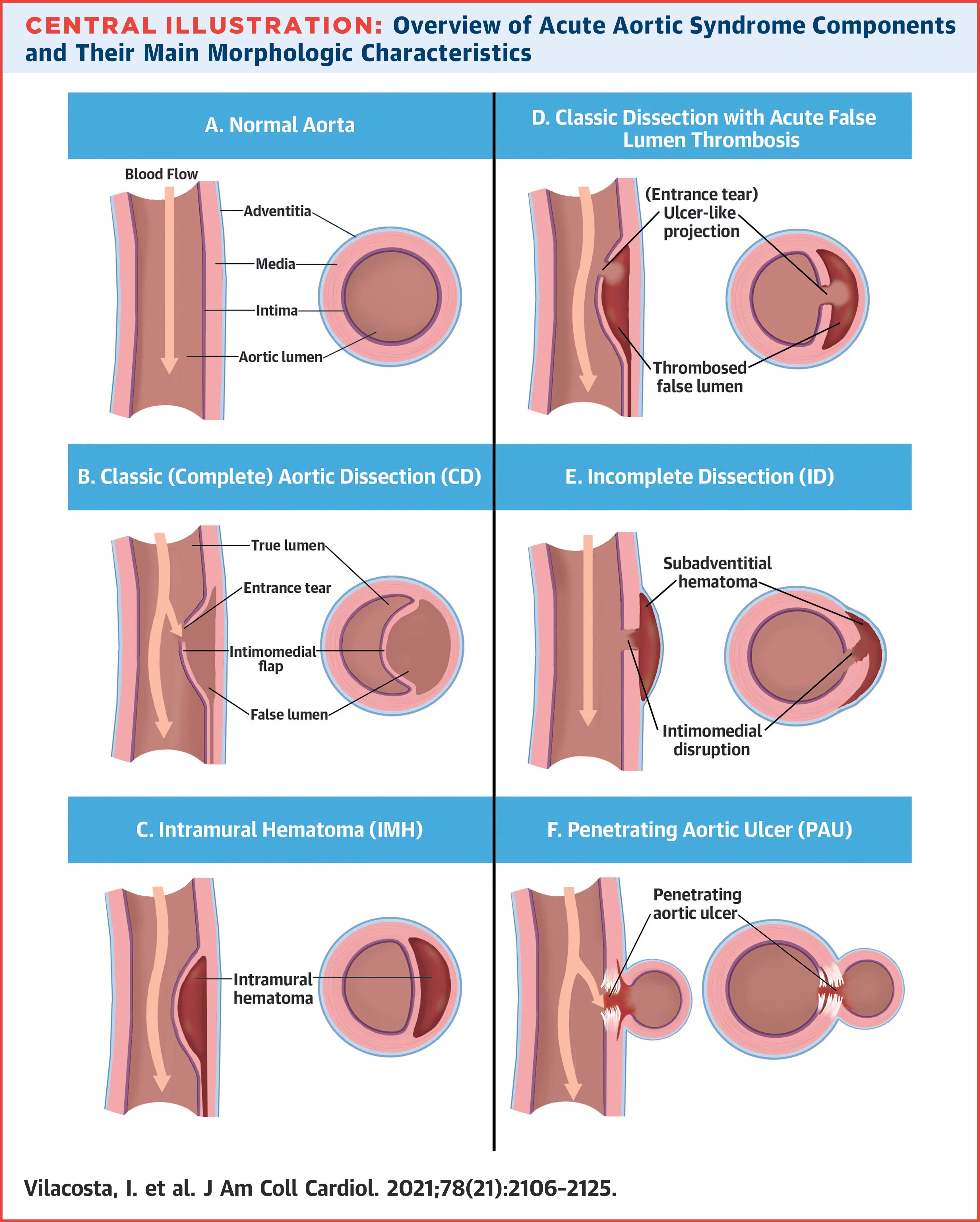
- Acute aortic syndrome embraces a cluster of 4 acute aortic conditions: classic dissection (CD), intramural hematoma (IHM), penetrating aortic ulcer (PAU), and incomplete dissection (ID)1
- From a surgical and prognostic standpoint, patients with AAS may be classified into 2 categories depending on the involvement (Stanford type A) or not (Stanford type B) of the ascending aorta.1
- Most recently, the Society for Vascular Surgery/Society of Thoracic Surgeons considers as type B AAS any aortic dissection with an entry tear originating distal to the ostium of the innominate artery1
Differential Diagnoses
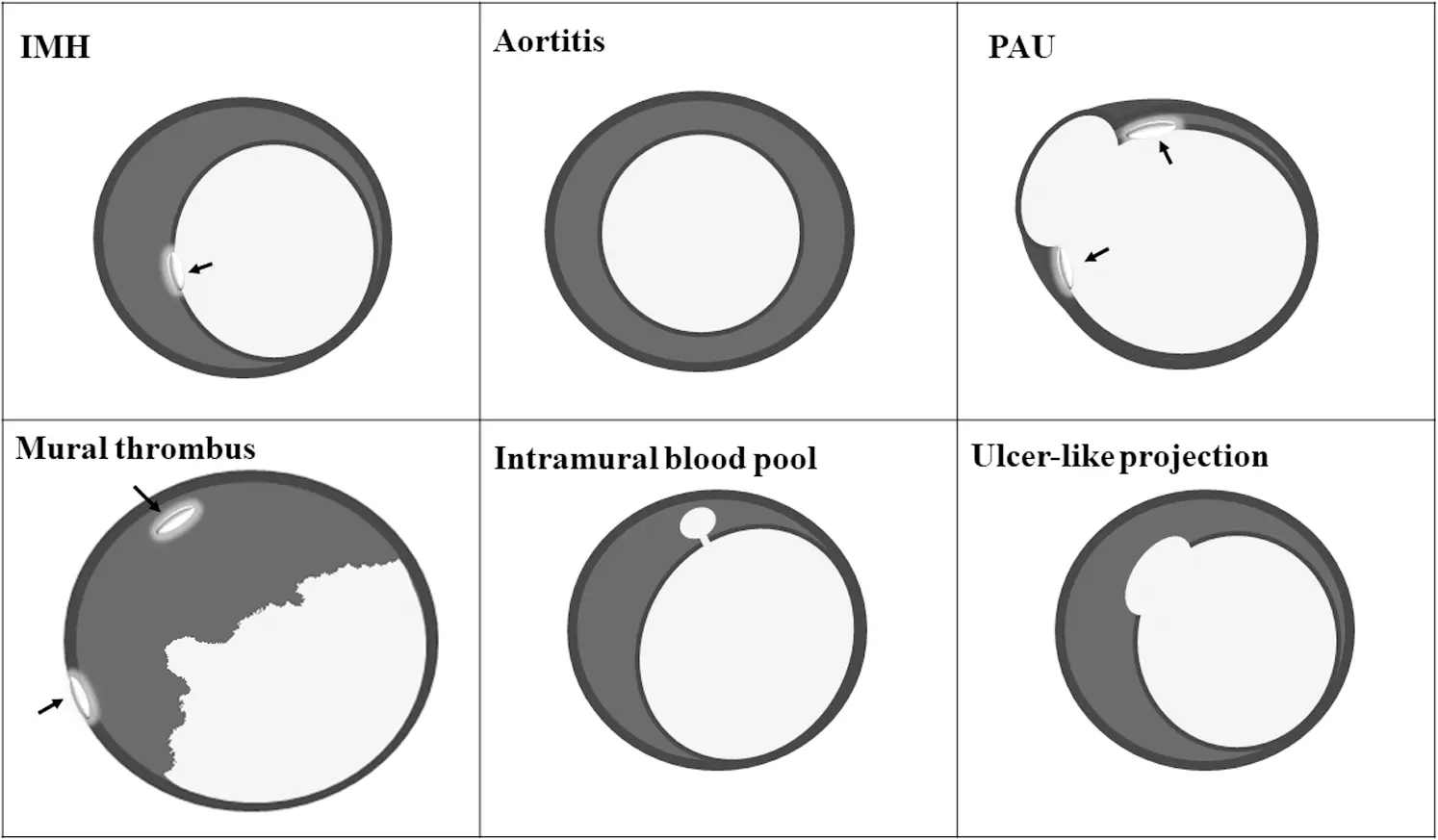 Figure caption: Acute Aortic Syndrome Computed Tomography Differential Diagnosis - Schematic representation of computed tomographic (CT) scans of the aorta of patients with acute aortic syndrome (AAS) and related entities. In intramural hematoma (IMH), calcium is displaced inwards, whereas in a dilated aorta with mural thrombus, calcium is located along the outer aorta border or within the thrombus. Aortic wall thickening is crescentic in IMH, whereas it is usually circumferential in aortitis. Ulcer-like projection (ULPs) have a wide communication with the aortic lumen, whereas intramural blood pools (IBPs) have a tiny communication. Both ULPs and IBPs are found in patients with IMH and are not usually accompanied by calcium deposits. Aortic wall deformation and calcified plaques are typically seen in patients with penetrating aortic ulcers (PAUs). Notice the calcium position (arrows) in each entity.1
Figure caption: Acute Aortic Syndrome Computed Tomography Differential Diagnosis - Schematic representation of computed tomographic (CT) scans of the aorta of patients with acute aortic syndrome (AAS) and related entities. In intramural hematoma (IMH), calcium is displaced inwards, whereas in a dilated aorta with mural thrombus, calcium is located along the outer aorta border or within the thrombus. Aortic wall thickening is crescentic in IMH, whereas it is usually circumferential in aortitis. Ulcer-like projection (ULPs) have a wide communication with the aortic lumen, whereas intramural blood pools (IBPs) have a tiny communication. Both ULPs and IBPs are found in patients with IMH and are not usually accompanied by calcium deposits. Aortic wall deformation and calcified plaques are typically seen in patients with penetrating aortic ulcers (PAUs). Notice the calcium position (arrows) in each entity.1
Footnotes
-
Vilacosta I, San Román JA, di Bartolomeo R, Eagle K, Estrera AL, Ferrera C, Kaji S, Nienaber CA, Riambau V, Schäfers HJ, Serrano FJ, Song JK, Maroto L. Acute Aortic Syndrome Revisited: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021 Nov 23;78(21):2106-2125. doi: 10.1016/j.jacc.2021.09.022. PMID: 34794692. ↩ ↩2 ↩3 ↩4