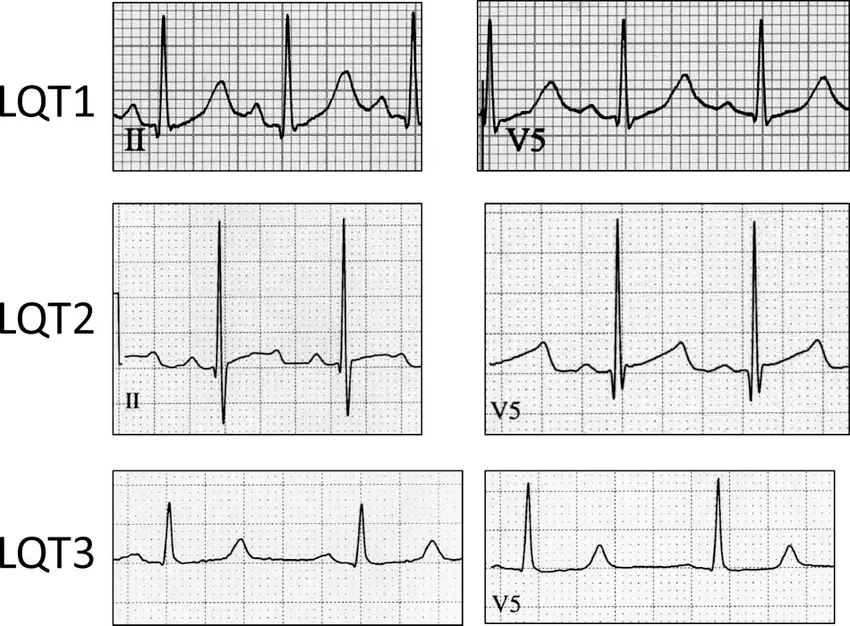
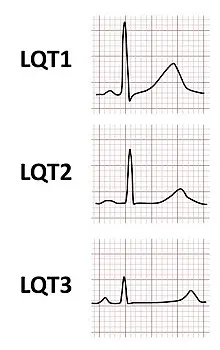
- Loss of function mutations in IKs and IKr prolong QT interval and produce LQTS1 and LQT2, respectively.
- The appearance of T wave can be a clue to type of LQTS

Diagnosis
Genetic testing
TODO
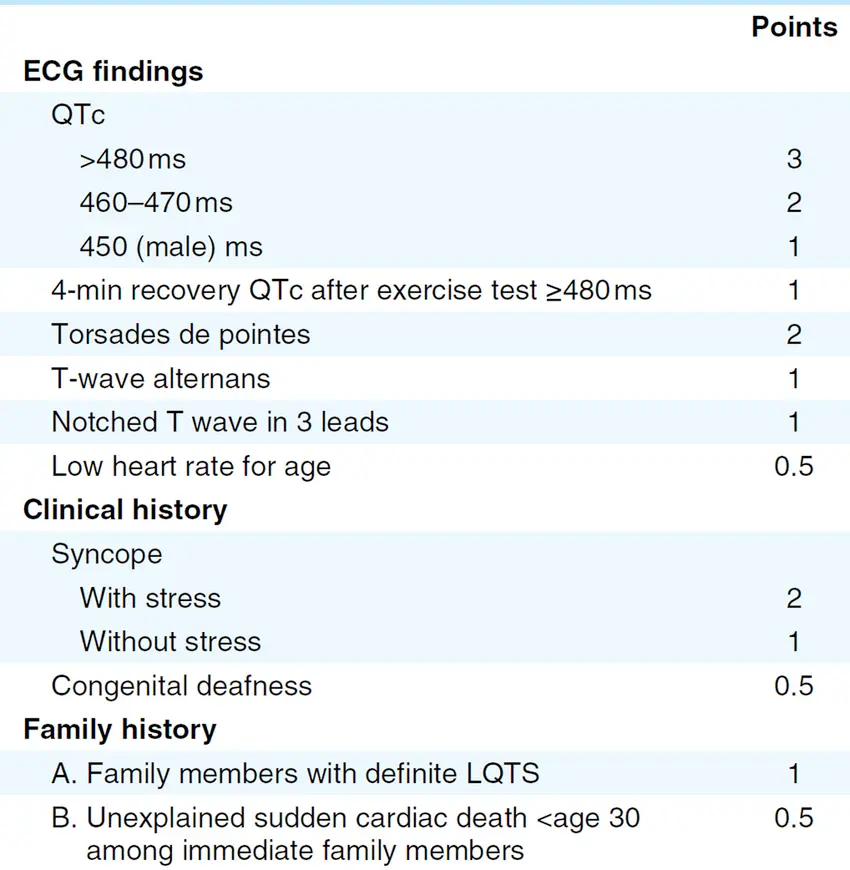
Schwartz score
- Schwartz score ≥3.5 carries a specificity of 99% for the diagnosis of LQTS.
- Genetic testing is recommended in those with Schwartz score ≥3.
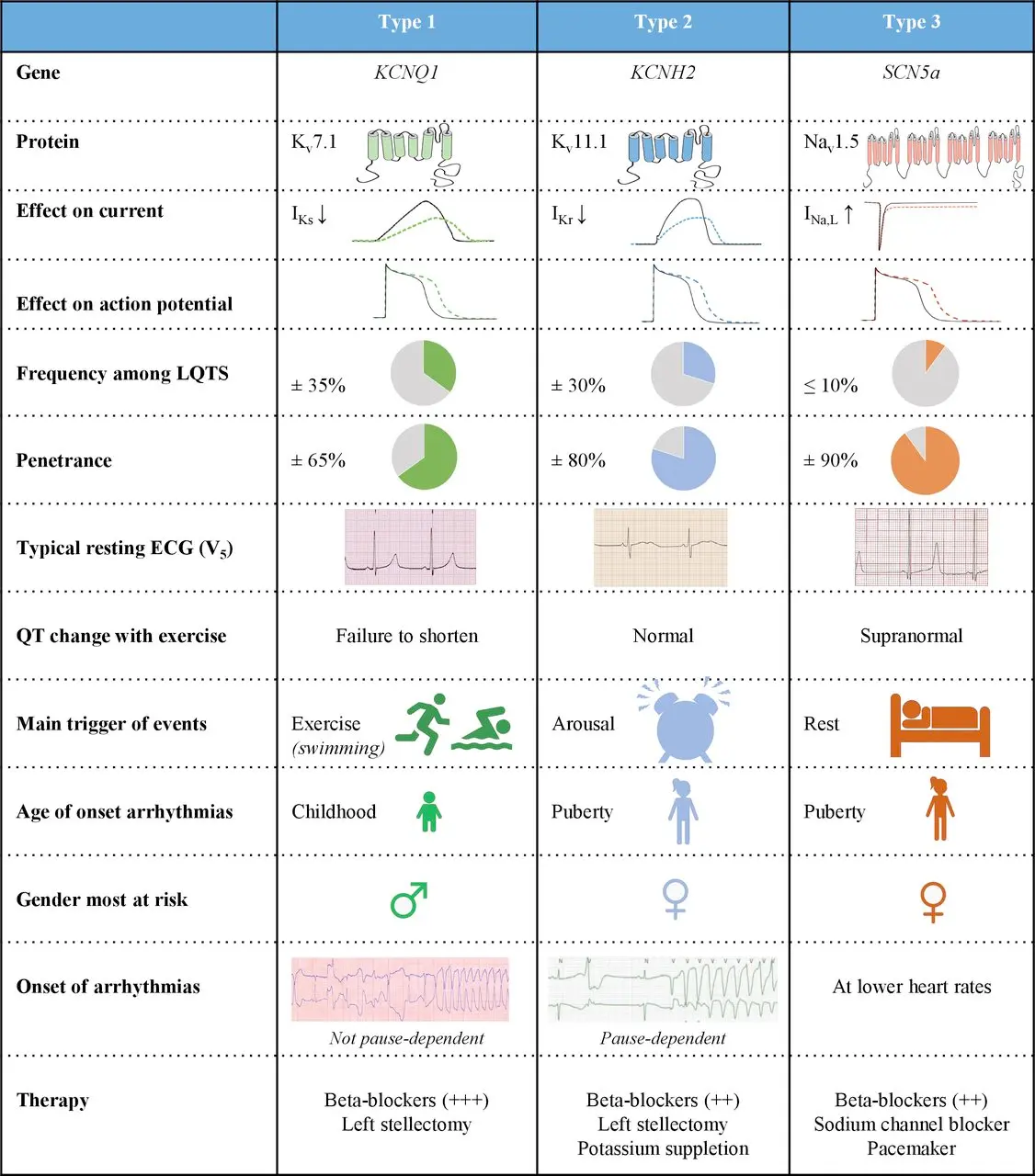
LQTS Type 1
LQTS Type 2
- Caused by a loss of function mutation → blockage of IKr channel
- Most common cause of drug-induced prolonged QT syndrome as many drugs are IKr blockers
- Second most common of LQT subtypes (25-30%)
- Exacerbated by auditory stimuli 🔊
- Events caused by alarm clocks, startle response, exercise
- Responsive to treatment with BBs and exercise restriction
- ICD indicated for:
- female patients with LQT2
- QTc > 500ms
- history of syncope/SCA
- 📝 Treating a patient with K-channel blockers like sotalol or dofetilide is like giving someone LQTS type 2, i.e. like block IKr channels.
LQTS Type 3
- Caused by gain of function of INa (SCN5a)
- Third most common of LQT subtypes (5-10%), considered most lethal
- Exacerbated by bradycardia, sleep
- Events only occur during sleep, so no warning signs, often present with SCA
- Responsive to treatment with BBs and exercise restriction, less so than LQT1, new data suggest role for ranolazine, mexiletine
- Diagnostic testing with suspected ECG and genetic testing
- ICD indicated for all patients with LQT3