Warning
The Mean QRS Vector, “Axis”, and Ventricular Hypertrophy cannot be determined accurately in the presence of Bundle Branch Block.
- RBBB and LBBB are specific varieties of interventricular conduction delay (IVCD)
- Caused by a block (of conduction) in the Right or in the Left Bundle Branch. The blocked Bundle Branch delays depolarization to the ventricle that it supplies.
- QRS > 0.12 secs, i.e. > 3 small squares
-20241220132421455.webp)
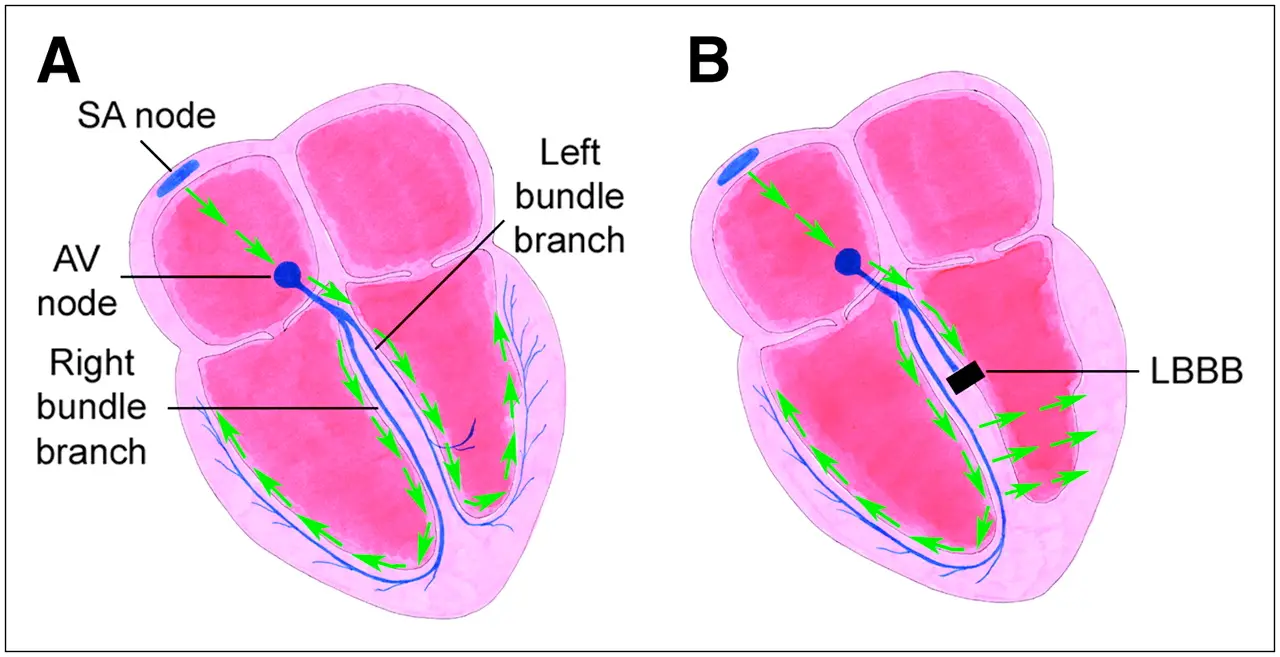 Figure source
Figure source
- LBBB almost immediately divides into 3 fascicles after splitting off from the His bundle. Hence, why if you see LBBB, it suggests a diffuse pathological process instead of a localized one.
- In the presence of complete LBBB, there is a significant delay between activation of the interventricular septum and activation of the left ventricular (LV) free wall 1
- ![[Left Bundle Branch Block LBBB-1747153456256.webp]]
- Where is the block located? 2
- Almost half the time, a “LBBB” is actually a left intrahisian block
- ![[Left Bundle Branch Block LBBB-1747152781961.webp|553x348]]
- ![[Left Bundle Branch Block LBBB-1747152858210.webp]]
- LBBB itself causes disordered LV contraction and in patients with poor systolic function, can worsen cardiac performance. (See Cardiac Resynchronization Therapy (CRT))
- In patients with LBBB and Heart Failure, CRT can help recoordinate ventricular contractions
- Prognosis:
- Younger patients with LBBB usually have no underlying heart disease, i.e. excellent prognosis
- Older patients, LBBB usually indicates presence of progressive heart disease (most commonly CAD, CM, or valvular heart disease)
- Widened, R-R’ appearance detected in leads V5 and V6
Complete versus Incomplete
- Complete LBBB
- QRS duration ≥120 ms
- Broad notched or slurred R wave in lateral leads (I, aVL, V5, and V6) and an occasional RS pattern in V5 and V6 attributed to displaced transition of QRS complex
- Absent Q waves in leads I, V5, and V6, but in the lead aVL, a narrow Q wave may be present in the absence of myocardial pathology
- R peak time >60 ms in leads V5 and V6 but normal in leads V1, V2, and V3, when small initial R waves can be discerned in the precordial leads
- ST and T waves usually opposite in direction to QRS
- Incomplete LBBB
- QRS duration between 110-119 ms
- LVH pattern
- R peak time >60 ms in leads V4, V5, and V6
- Absence of Q wave in leads I, V5, and V6
Comparison of LBBB ECG Criteria
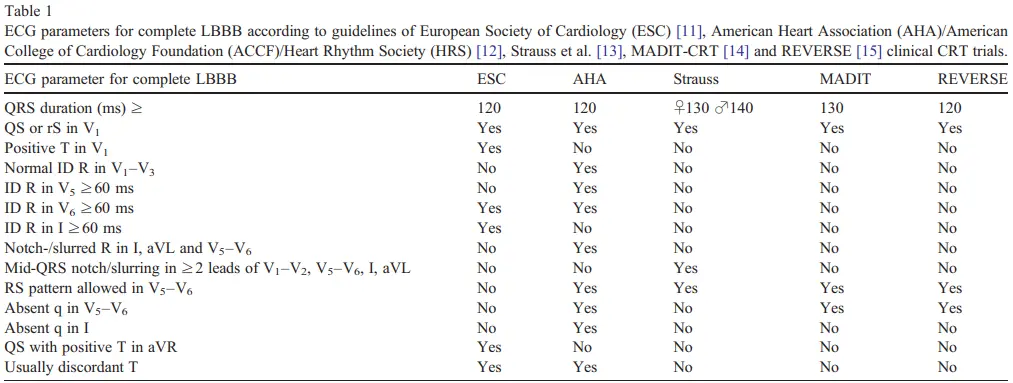 Table source: 3
Table source: 3
Strauss Criteria for Complete LBBB
- 1 propose stricter criteria for complete LBBB that include:
- QRS duration ≥140 ms for men and ≥130 ms for women
- Rationale: men have larger hearts that take longer to depolarize
- QS or rS in leads V1 and V2
- mid-QRS notching or slurring in ≥2 contiguous leads (of leads V1, V2, V5, V6, I, and aVL)
- The first notch represents the time when the electrical depolarization wave front reaches the endocardium of the LV (after proceeding through the septum). The second notch occurs when the depolarization wave front begins to reach the epicardium of the posterolateral wall.
- ![[Left Bundle Branch Block LBBB-1747153641789.webp]]
- QRS duration ≥140 ms for men and ≥130 ms for women
Footnotes
-
Strauss DG, Selvester RH, Wagner GS. Defining left bundle branch block in the era of cardiac resynchronization therapy. Am J Cardiol. 2011 Mar 15;107(6):927-34. doi: 10.1016/j.amjcard.2010.11.010. PMID: 21376930. ↩ ↩2
-
Upadhyay GA, Cherian T, Shatz DY, Beaser AD, Aziz Z, Ozcan C, Broman MT, Nayak HM, Tung R. Intracardiac Delineation of Septal Conduction in Left Bundle-Branch Block Patterns. Circulation. 2019 Apr 16;139(16):1876-1888. doi: 10.1161/CIRCULATIONAHA.118.038648. PMID: 30704273. ↩
-
van Deursen CJ, Blaauw Y, Witjens MI, Debie L, Wecke L, Crijns HJ, Prinzen FW, Vernooy K. The value of the 12-lead ECG for evaluation and optimization of cardiac resynchronization therapy in daily clinical practice. J Electrocardiol. 2014 Mar-Apr;47(2):202-11. doi: 10.1016/j.jelectrocard.2014.01.007. Epub 2014 Jan 6. PMID: 24444866. ↩