-
Related:
-
Saghir prefers to open this in
Load→TAVR(available in theOthertab)CPRbutton at top for curved planar reconstruction, which creates a vessel surf kind of thing in TerraRecon
-
After looking at the topogram, look at the Left atrial appendage delay image. This
Serieswill be called something likeLAA DELAY… -
Scroll through to make sure that the LAA fills appropriately with contrast.
-
The image
Seriesthat has the word “Multiphase” contains the actual gated heart study, i.e. obtained through all of the phases.- Open this study using a 4D workflow by Right clicking → Select
HEART→ SelectCardiac - 📝 will take a while to load because there are so many images.
- Open this study using a 4D workflow by Right clicking → Select
-
We will begin by looking at the LV and RV size and function
- LV: move your crosshairs to the basal-mid of the LV with the crosshair pointing towards the apex of the LV in 2 planes
- Press Play → you’ll see your 2 chamber, 4 chamber, and SAX views
-
There is a button Dr. Hutt showed that estimates LVEF among the options on the right-side of the screen.
- ⚠️ As a sanity check, make sure that it is tracking well though.
-
Next, look at the AV and assess open/close
-
You will close the Multiphase series and load the
SYSTOLICandCTA_CAPseries next. To open both you will holdCtrland select both → Right click and selectHEART→ 4DTAVI.
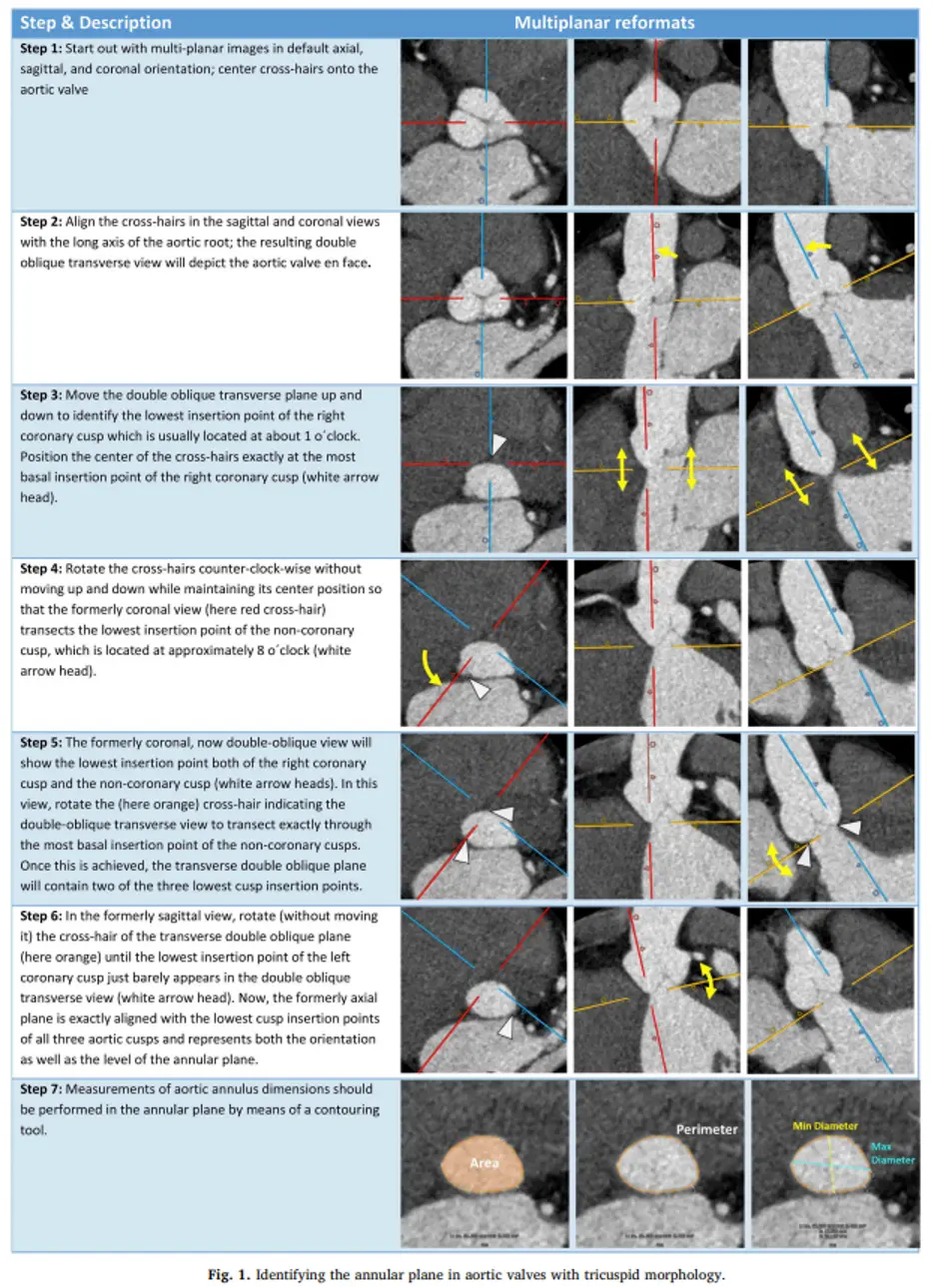 Figure source: 1
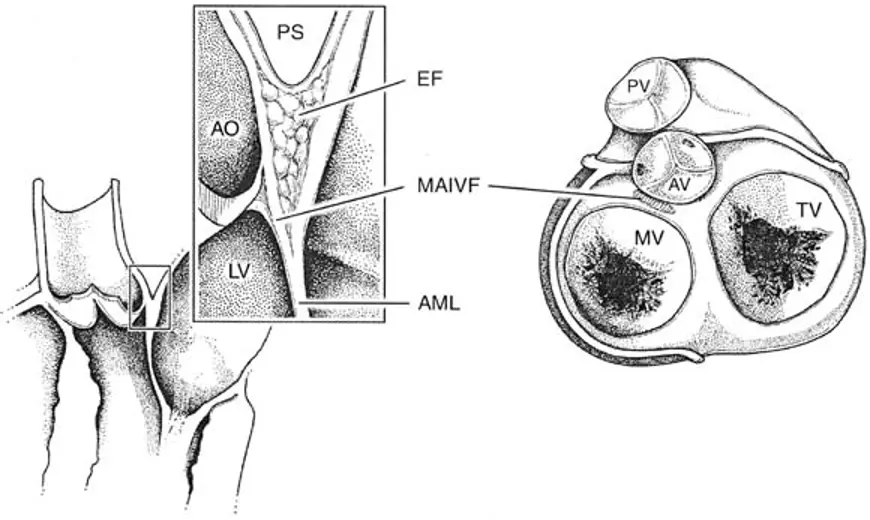
Figure source: 1
Estimate LVEF
- On the Right top column there is an LVEF module that you can use to estimate LVEF
- Dr. Saghir said it works well about ~80% of the time.
TAVI “Landing Zone”
- The TAVI “landing zone” comprises the valve cusps, aortic annulus and LVOT.1
- The device landing zone is in close spatial relationship with the conduction system ⚡ which may be compressed and damaged, causing AV block and need for pacemaker implantation especially in the context of severe calcification of the subannular device landing zone, with this effect amplified in the presence of pre-existent Right Bundle Branch Block.1
Calcium in the “Landing Zone”
- The presence of severe calcification of the LVOT and aortic valve is associated with increased risk of paravalvular regurgitation particularly when calcium protrudes into the LVOT.1
- The region below the non-coronary and the left coronary cusps, including the intervalvular fibrosa, is most frequently affected.1
- In clinical practice, the description of annular (within annular plane) and sub-annular (upper 4–5mm of the LVOT where device gets into contact) calcification is almost exclusively performed in a subjective, qualitative fashion graded as none, mild, moderate, severe based on the circumferential extent, the depth of extension inferiorly into the LVOT and the thickness of the calcification projecting radially into the LVOT.1
- Annular and sub-annular calcification should be described as crescent/flat/adherent or protruding as well as its relation to the aortic cusps.1
Footnotes
-
Blanke P, Weir-McCall JR, Achenbach S, Delgado V, Hausleiter J, Jilaihawi H, Marwan M, Norgaard BL, Piazza N, Schoenhagen P, Leipsic JA. Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI) / transcatheter aortic valve replacement (TAVR): An expert consensus document of the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2019 Jan-Feb;13(1):1-20. doi: 10.1016/j.jcct.2018.11.008. Epub 2019 Jan 7. PMID: 30630686. ↩ ↩2 ↩3 ↩4 ↩5 ↩6 ↩7