-
Seen if there is antegrade conduction through the bypass (accessory) pathway
-
“WPW pattern” is asymptomatic pre-excitation, whereas “WPW syndrome” involves symptomatic arrhythmia.
-
Characterized by:
- short PR interval
- PR interval < 120 ms
- Normal P wave vector (to exclude junctional rhythm)
- Prolonged QRS interval
- QRS duration > 100 ms
- Delta wave
- dependent on accessory pathway location and AV nodal conduction time
- short PR interval
-
The degree of pre-excitation depends on several factors:
- AV nodal conduction time
- the slower AV nodal conduction, the larger the delta wave
- the conduction velocity of the bypass tract
- rapid conduction velocity → more pre-excitation
- the refractory period of the bypass tract
- shorter RP → more pre-excitation
- proximity of the bypass tract to the SA node
- atrial impulses reach R-sided bypass tract earlier than a L-sided bypass tract; ∴ R-sided bypass tracts tend to have more pre-excitation
- AV nodal conduction time
-
⚠️ For someone with WPW, you won’t see the delta waves while they’re in SVT
-
![[AV Reentrant Tachycardia AVRT-1745549180943.webp]]
-
Concern of WPW progressing - ![[AV Reentrant Tachycardia AVRT-1745549218573.webp]]
Diagnosis
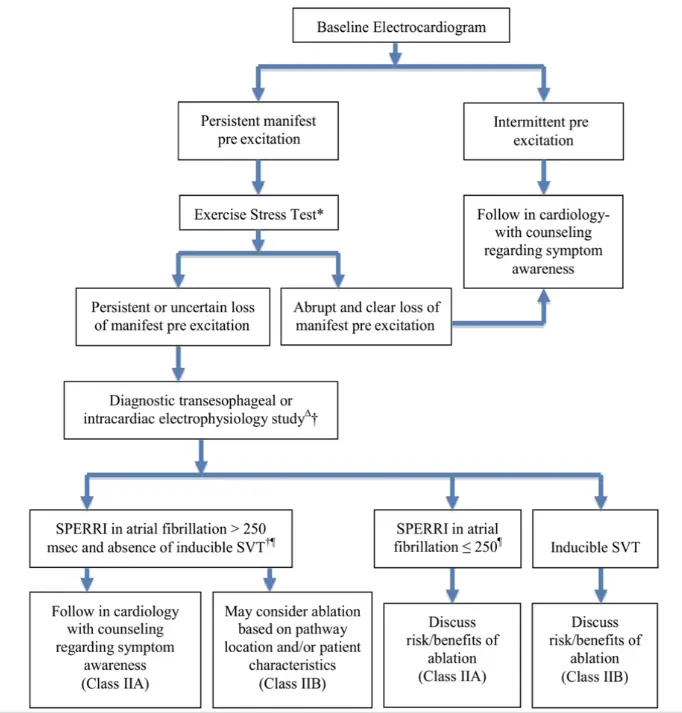
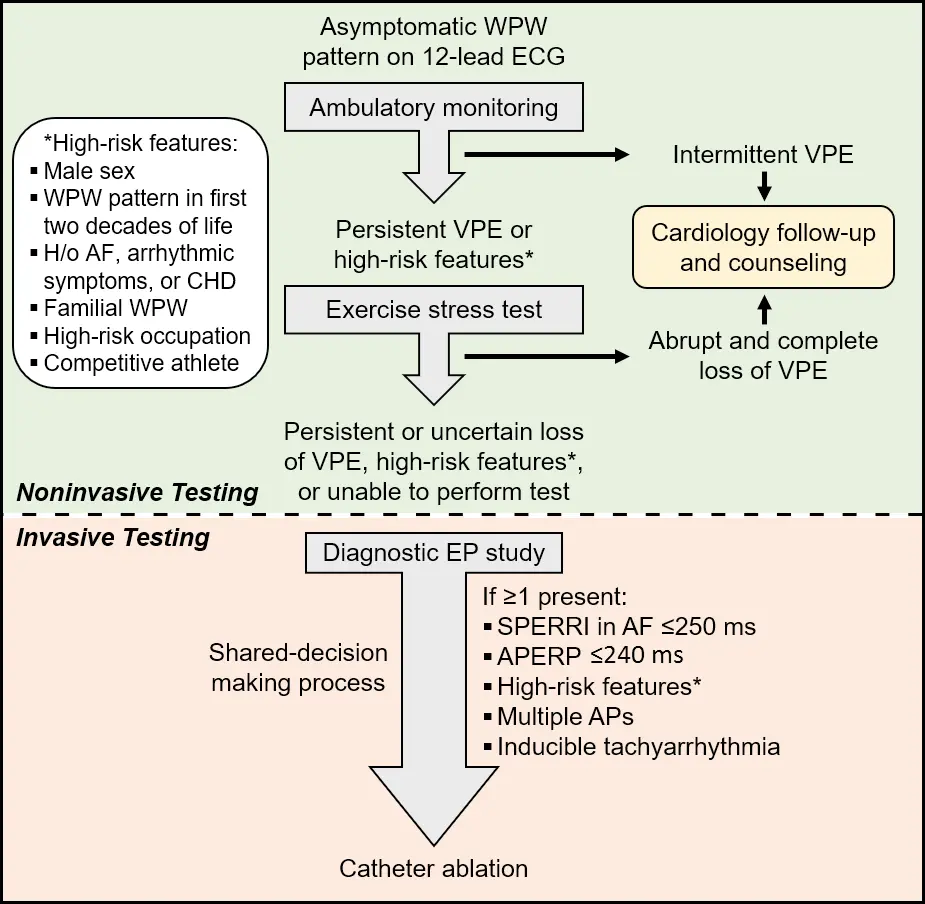
- Noninvasive testing is generally considered safe and should be considered in asymptomatic WPW patients. This includes standard 12-lead ECG, ambulatory monitoring, and exercise stress testing (EST).
Exercise testing
- A significant proportion of patients with ventricular pre-excitation remain asymptomatic yet at the risk of life-threatening arrhythmias.
- Intermittent ventricular pre-excitation during ambulatory monitoring or abrupt and complete termination of accessory pathway conduction during stress testing suggests a low-risk pathway.
- Shortest pre-excited RR interval (SPERRI) during atrial fibrillation <250 ms, or accessory pathway effective refractory period <240 ms suggest a high-risk pathway.
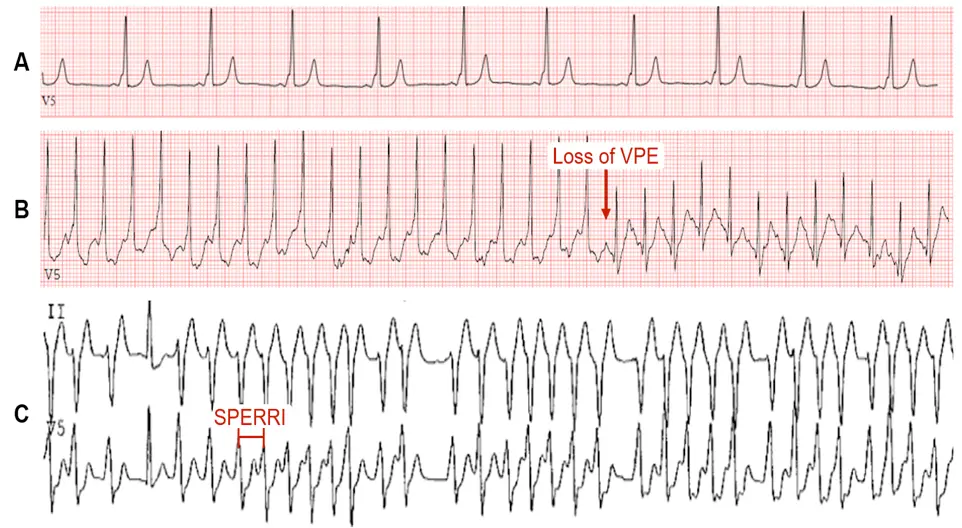 1A: Typical WPW preexcitation pattern manifesting as a short PR interval, delta wave, and wide QRS complex. 1B: Loss of ventricular preexcitation (VPE) during noninvasive testing.1C: Noninvasive shortest preexcited R-R interval (SPERRI) measurement during rapid preexcited AF that can potentially precipitate ventricular fibrillation. (Source)
1A: Typical WPW preexcitation pattern manifesting as a short PR interval, delta wave, and wide QRS complex. 1B: Loss of ventricular preexcitation (VPE) during noninvasive testing.1C: Noninvasive shortest preexcited R-R interval (SPERRI) measurement during rapid preexcited AF that can potentially precipitate ventricular fibrillation. (Source)
Wolf-Parkinson-White Syndrome
- When you have arrhythmia ⚡ or Sx related to accessory pathway
- In the absence of a documented tachyarrhythmia or related symptoms, the ECG findings alone are referred to as WPW pattern.
- Wolff-Parkinson-White (WPW) syndrome affects 0.1-0.3% of the general population.
- The characteristic ECG features in WPW Syndrome are:
- shortened PR interval (<120 ms):
- slurred QRS upstroke (delta wave)
- prolonged QRS duration (>120 ms)
- ☠️ The chief fear of both WPW syndrome and pattern is the risk for sudden cardiac death (SCD) – presumed to result from rapid VPE precipitating VFib.
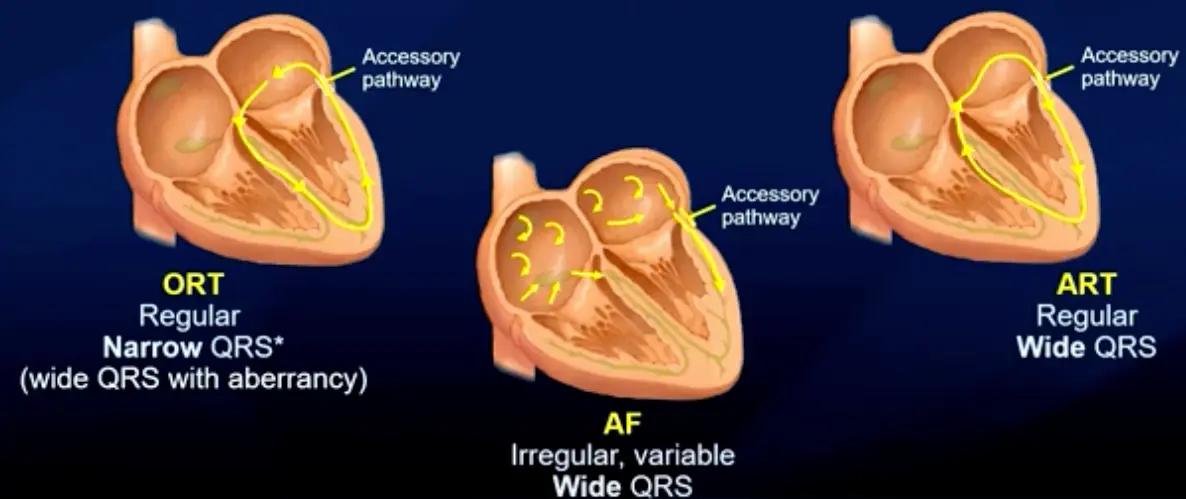
- 3 major arrhythmias:
- ORT
- regular
- narrow QRS (wide QRS if aberrancy)
- Antidromic AVRT
- regular
- wide QRS
- AFib associated with an accessory pathway
- ORT