| High Intensity | Moderate Intensity | Low Intensity | |
|---|---|---|---|
| LDL-C Lowering | ≥50% | 30%–49% | <30% |
| Statins | Atorvastatin (40 mg) 80 mg Rosuvastatin 20 mg (40 mg) | Atorvastatin 10 mg (20 mg) Rosuvastatin (5 mg) 10 mg Simvastatin 20–40 mg | Simvastatin 10 mg |
| Pravastatin 40 mg (80 mg) Lovastatin 40 mg (80 mg) Fluvastatin XL 80 mg Fluvastatin 40 mg BID Pitavastatin 1–4 mg | Pravastatin 10–20 mg Lovastatin 20 mg Fluvastatin 20–40 mg | ||
| Table source: Table 3 of 1 |
-
Dr. O’Keefe is not a fan of Atorva 80 mg b/c side effects of statins are dose-dependent.
- You can get rhabdo with high doses of statins. Dr. O’Keefe gave an example of post-transplant patient on Atorva 80 who got rhabdo and died a few months later.
- Delta between 40 mg and 80 mg of atorva is 48% → 51% reduction (delta is only 3%)
-
Atorva is the 🌟
- less nephrotoxicity compared to rosuvastatin
-
Rule of thumb: 6% reduction when doubling a statin dose. Better off adding ezetimibe: zetia on its own 16% reduction, zetia + statin (synergistic effect): 25% reduction.
-
Newborn baby LDL is 25-30 mg/dL. Hunter/gatherers have also been studied and have like 40-50 mg/dL.
- You don’t want a 0 LDL! Cholesterol is an important molecule, so you need some.
-
Dr. O’Keefe gets nervous getting someones LDL < 30
-
Side effects are not related to LDL level, rather related to statin dose.
-
⚠️ Statins are contraindicated in pregnancy 🤰and lactation
-
📝 At equivalent statin doses, Asians achieve greater LDL lowering than Westerners
- ∴ Consider starting with lower dose (1/4 dose) in Asians
-
Mnemonic for statin side effects “LIPITOR”:
- Liver effects
- Increased blood sugar
- Pain (muscles)
- Impaired memory
- Tiredness/Fatigue
- Other (headaches)
- Rhabdomyolysis
-
SAMSON trial (BMJ, 2021)
- 200 statin intolerant patients; “n-of-1” experiments
- Compared atorva 20 mg vs placebo
- Intolerable muscle sx: 9% in statin group discontinued, 7% discontinued placebo
-
FDA did put out a warning on “brain fog” with statins, but meta-analysis showing ↓ Alzheimer’s Risk 32%
-
Dr. O’Keefe: “when I start someone on a statin, I also start them on CoQ10.”
- If patient c/o myalgias, he’ll increase the dose of CoQ10
-
Pitavastatin
- a “cool” statin
- Not as strong as atorva
- 4 mg dose 20 mg of atorva
- Unlike atorva, rosuva, simva, Pitavastatin less likely to induce DM in patients. If anything pitava can lower A1c by 0.1%
High-Intensity Statins
- Rosuvastatin 20-40 & Atorvastatin 40-80 mg
- Maximally tolerated statin still the foundation
- ↓ LDL-C ~50%
- Can get creative to identify “maximally tolerated” to manage intolerance
- Symmetric myalgias in large proximal muscle groups may indicate true statin intolerance; RARE
- SAMSON trial - 90% of muscle symptoms attributed to “nocebo effect”
- Rule out/correct other causes of muscle symptoms: hypothyroidism, vitamin D deficiency, exercise
- Hydrophilic statins potentially less muscle symptoms (rosuvastatin, pravastatin)
- Up to 90% of initially intolerant do fine with re-challenge
- Allow 2-4 week wash out
- Symmetric myalgias in large proximal muscle groups may indicate true statin intolerance; RARE
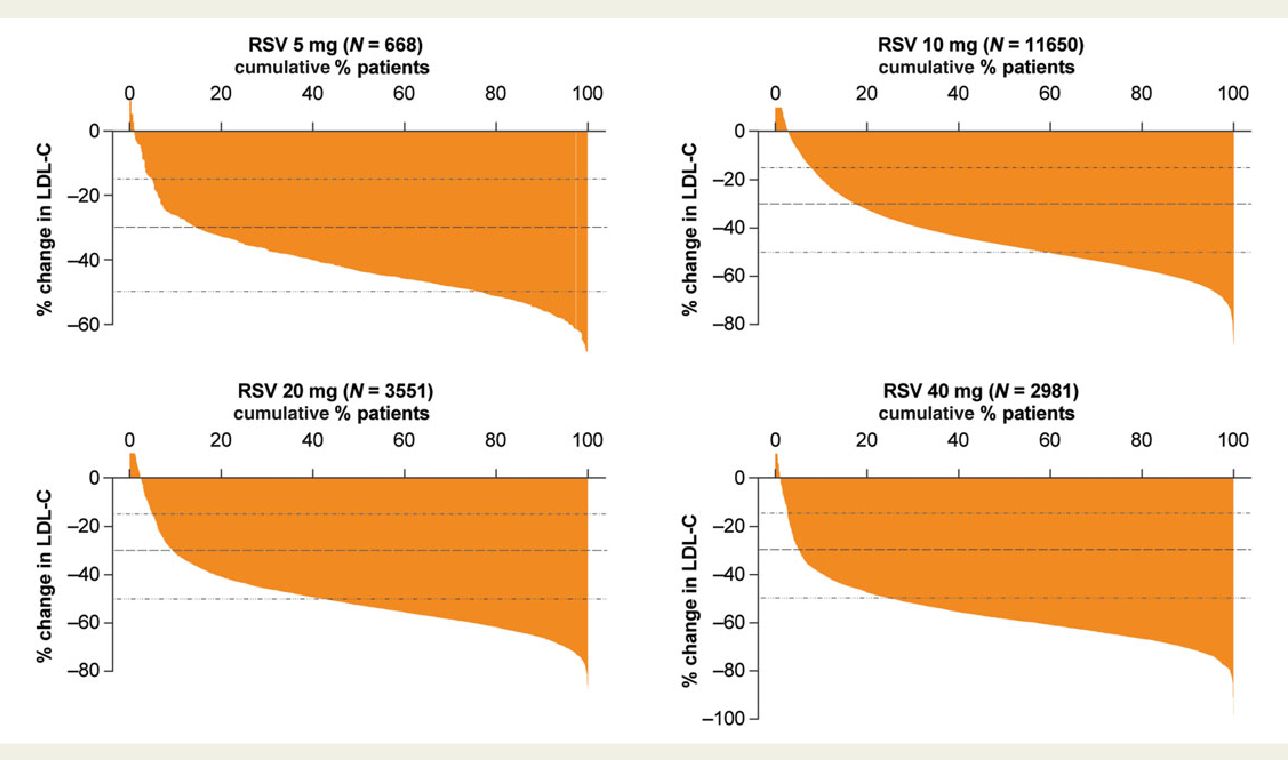
Variability in individual response to statins
Drug-Drug Interactions
Simvastatin
- Risk of myopathy, including rhabdomyolysis, is ↑ by concomitant administration of:
- CCBs Verapamil or Diltiazem
- 📝 Simvastatin dose should not exceed 10 mg/day!
- Amiodarone, Amlodipine or Ranolazine
- 📝 Simvastatin dose should not exceed 20 mg/day!
- CCBs Verapamil or Diltiazem
Footnotes
-
Grundy, S, Stone, N, Bailey, A. et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. JACC. 2019 Jun, 73 (24) 3168–3209. https://doi.org/10.1016/j.jacc.2018.11.002 ↩