- “Idiopathic VT” is essentially VT that occurs in the setting of a structurally normal heart, i.e. absence of ischemia, valvulopathies, or other cardiomyopathies, etc.
- Catheter ablation can be used to treat and potentially provide a cure in patients that are intolerant to medications or when these are ineffective.
- Patients generally are not at an increased risk of sudden death and do not require implantation of an ICD.
- Idiopathic VT can arise from anywhere in the heart, but certain regions are more common than others.
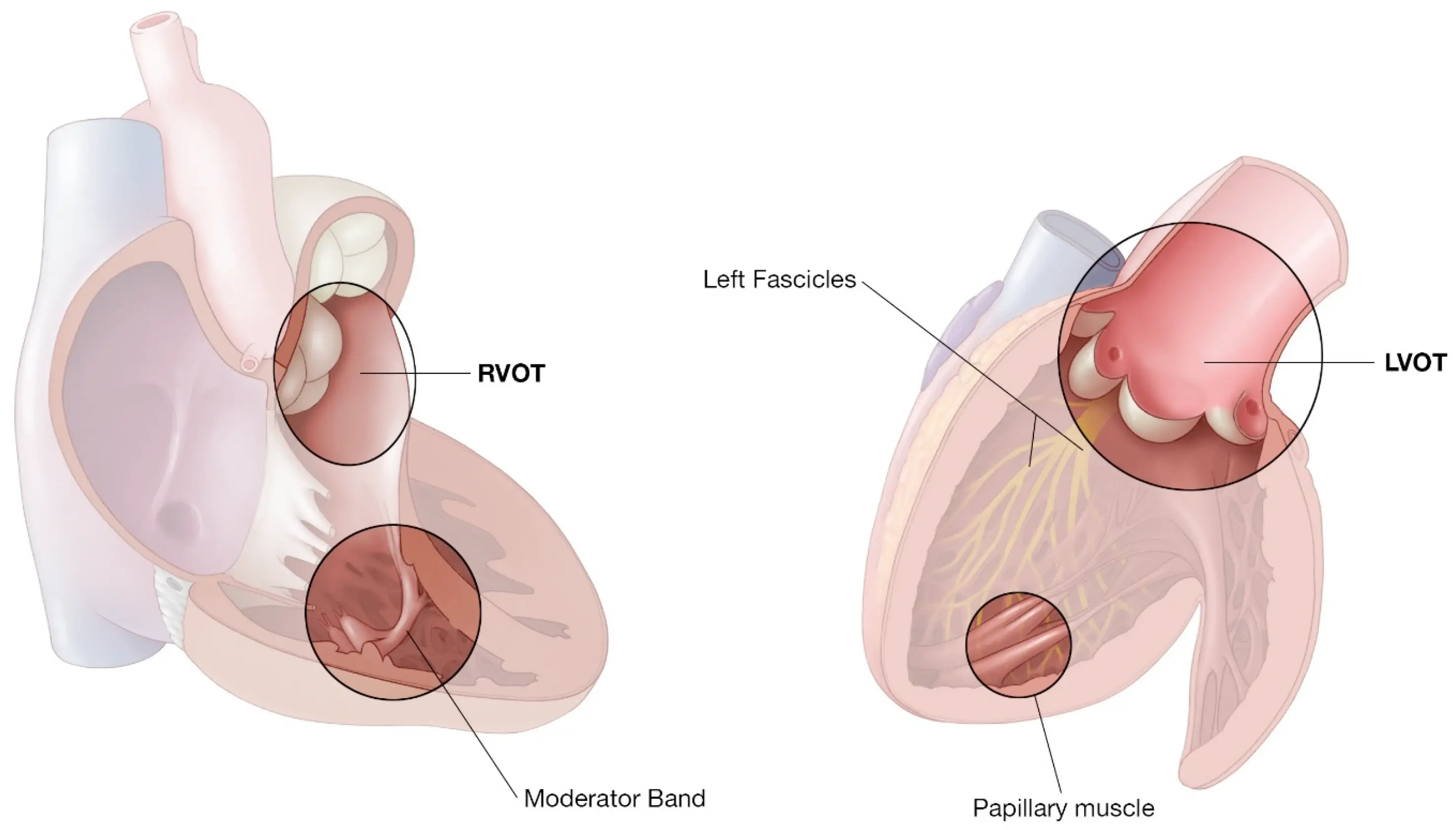
Outflow Tract Tachycardias
RVOT VT
- Structurally normal hearts
- Rarely associated with SCD
- Most of these patients have palpitations, lightheadedness, and syncope.
- Triggers
- Men: exercise or catecholamine-related
- Women: hormonal, e.g. can be around perimenopausal or peri-pregnancy periods.
-
10% of arrhythmia burden can be associated with development of cardiomyopathy
- Keep 👀 out to detect for LV dysfunction
- Mechanism
- DADs: at slower rates, there is a little calcium overload in the cell. At faster HR, and one of these calcium overload reach the activation threshold → generates a QRS complex.
- Work-up
- Exclude ARVC as a cause of the arrythmia
- Management
Papillary Muscle VT
- Papillary muscle cells develop pacemaker-like current.
- Mechanism