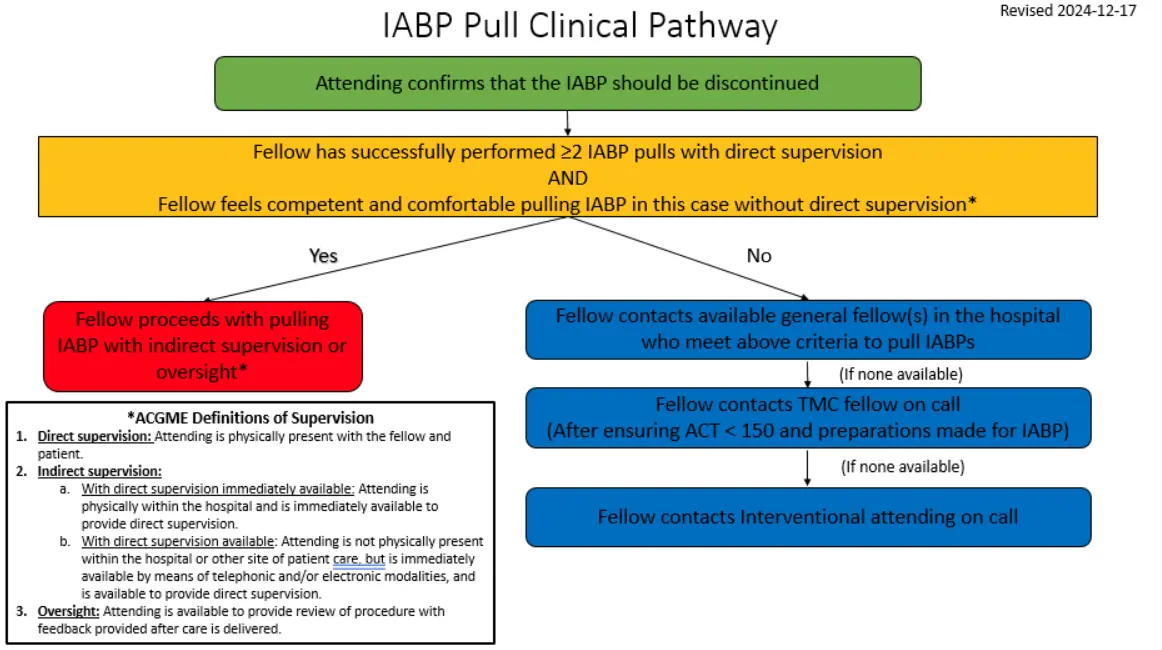
In the very rare situation that attending requests IABP to be pulled after 5 pm for some reason (e.g., ACT didn’t come down < 150 during the day, etc.),
you may pull if you’ve done 2 supervised pulls already and you feel comfortable doing it on your own
if not, call UH fellow on call if they are comfortable and certified
if UH fellow is a no-go, then call interventional attending on call
If you deem the patient hemodynamically improved and no longer needs IABP, change IABP from 1:1 to 1:2 or 1:3 (or gradually reduce inflation volumes down to 50% at 1:1) over 4-5 hours and re-assess clinical condition, UOP, Swan numbers, and labs in an hour.
If numbers/clinical status remains stable, change back to 1:1 and stop heparin drip.
Notify nurse and Jana Doree or her equivalent about plans to pull the IABP. Get equipment:
suture removal kit
gauze
towels
sterile gloves
chlorhexidine prep
Check ACT in 1-2 hours and repeat sequentially until ACT < 150 ms.
Once ACT is below 150 ms, OK to pull IABP.
Give fentanyl 25 or 50 mcg.
Palpate the pulse and feel confident you know how it courses.
Sometimes, to palpate it you may need to be on standby briefly.
Confirm with Doppler that you are able to compress the femoral artery.
Once you have a good handle on the pulse, you can begin.
Call time out, assess vitals. Wear sterile gloves and clean the area with chlorhexidine prep. Remove tape, sutures.
Turn off IABP.
Withdraw IABP catheter until the balloon reaches the sheath, then pull sheath and IABP out as one unit. Classical teaching is to let a few squirts of blood out first (optional). Then, hold firm pressure proximal to IABP insertion site.
Hold occlusive pressure (should not be able to Doppler DP signal) for 5 minutes.
Then a qualified nursing assistant can take over for the next 25 minutes. If at any point, loss of hemostasis, restart timer.
Document brief procedure note. There is a code for IABP removal that you can associate with your procedure note.
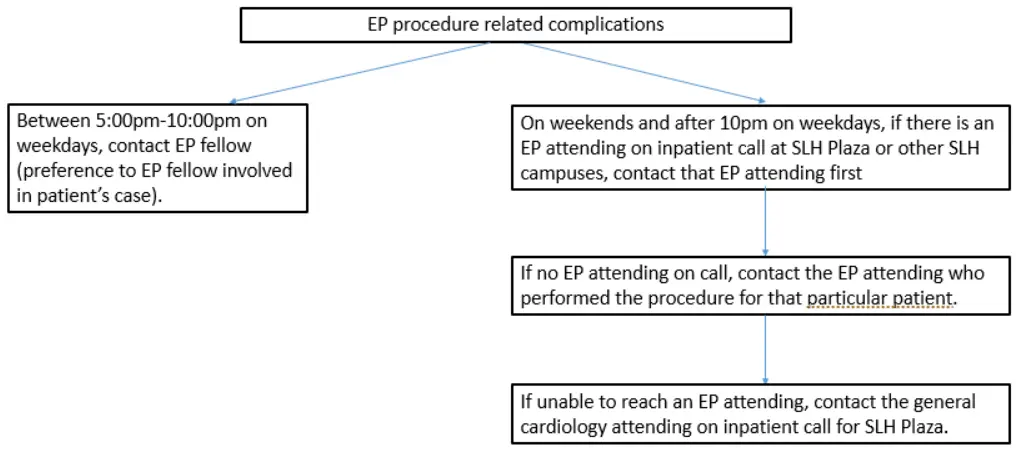
EP Procedural Complications
If weekday before 10 pm, call EP fellow (first preference is to call the fellow more involved in the patient’s care)
If weekday after 10 pm or weekend, call any EP attending on call at any of the SLH hospitals.
If no EP attending on call, call the EP attending who did the procedure.
If they’re not available, call general cardiology attending on call.
Cath Complications
Minor bleeding (hemodynamically stable, hemostasis with manual compression (general rule of thumb is to apply pressure for 3-5 minutes per French), hematoma < 10 cm) →
clinical monitoring
obtain imaging (arterial doppler, CT non-contrast can rapidly diagnose retroperitoneal hematoma though doesn’t show site of extravasation)
Major bleeding (hemodynamically unstable, no hemostasis despite appropriate manual compression; expanding hematoma or retroperitoneal hematoma) →
📞 Call interventional attending on call (interventional fellow not part of algorithm);
IVF/transfuse
Move to ICU
Angiogram or vascular intervention per interventional attending