- Sequence of review
- General
- Coronary dominance
- Coronary arteries for obstruction/stenosis
- Cardiac chambers
- Pericardium
- Great Vessels
- Lungs
- Mediastinum
- Upper abdomen
- Chest wall
- Bony structures (bone window)
- Sternum
- Ribs
- Vertebral bodies
- General
Coronary evaluation
- As a first pass, Dr. Maroules likes to switch to MIP view (e.g. slab thickness of 5 mm) and investigate the coronary anatomy
- Is the LM coming off of the Left sinus? Is the RCA coming off of the Right sinus? Any anomalous coronary arteries?
- LM bifurcation (into LAD, LCx) or trifurcation (into LAD, LCx, ramus)
- When evaluating coronary arteries, we are evaluating for: (See CAD-RADS)
- plaque
- stenosis
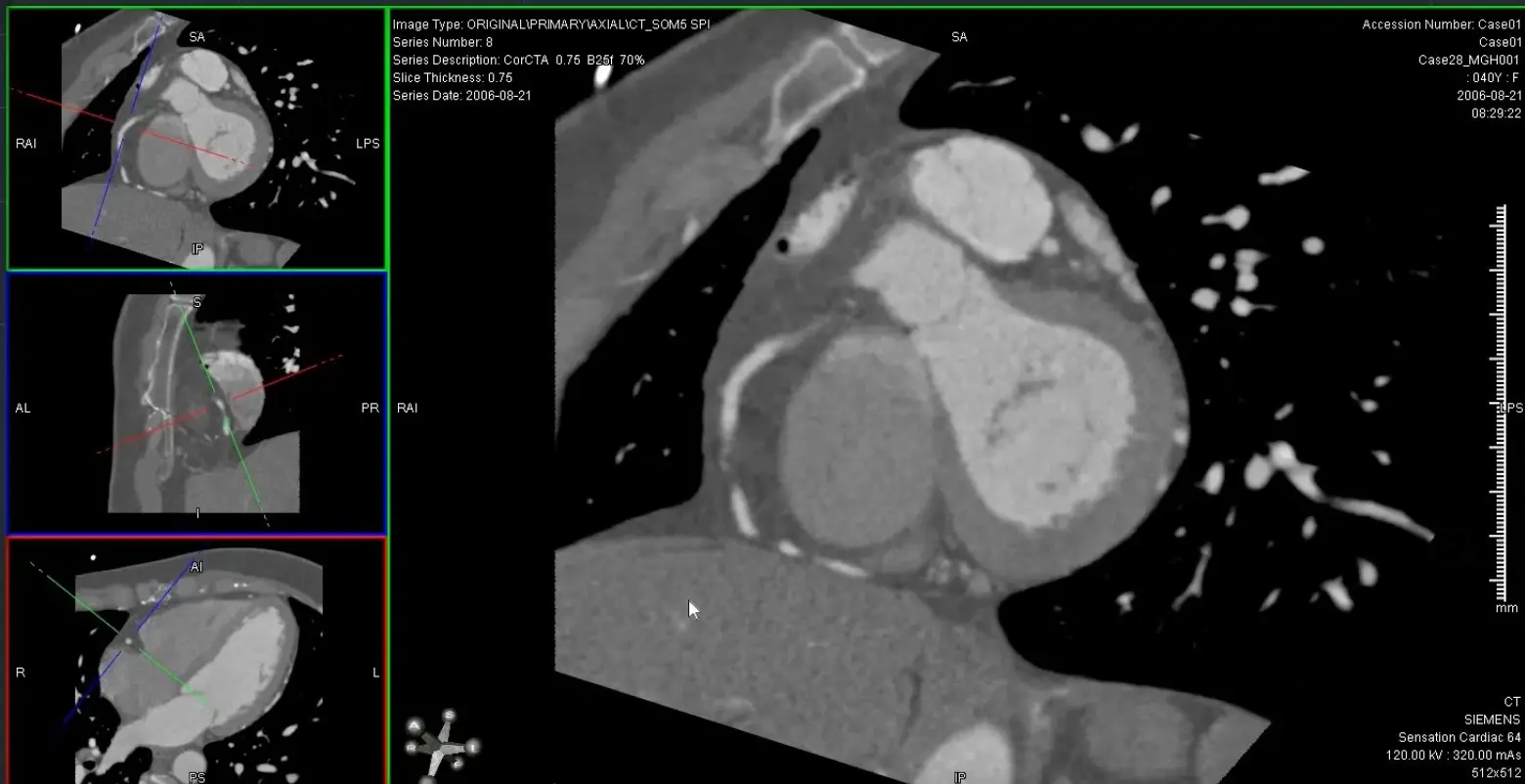
- Generate orthogonal views of coronary arteries using MPR (e.g. 0.5 mm thickness) to be able to evaluate luminal narrowing
- → Align 2 view through the long axis
- → Then double click on the remaining plane to see the SAX and evaluate for luminal stenosis
- Use the SAX images to measure 📐 luminal stenosis
- ⚠️ for vessels <1.5 mm in diameter, it is difficult to quantify and grade stenosis, but calcified plaque is usually apparent even within these small vessels.
- Dr. Maroules likes to follow it back with a backward pass (i.e. distal→proximal) to make sure he didn’t miss anything
- LAD
- Likes to travel in the anterior interventricular groove
- Diagonal branches like to course along the anterior and anterolateral LV
- You will see small septal perforators diving into the myocardial
- You will see diagonal branches coming off
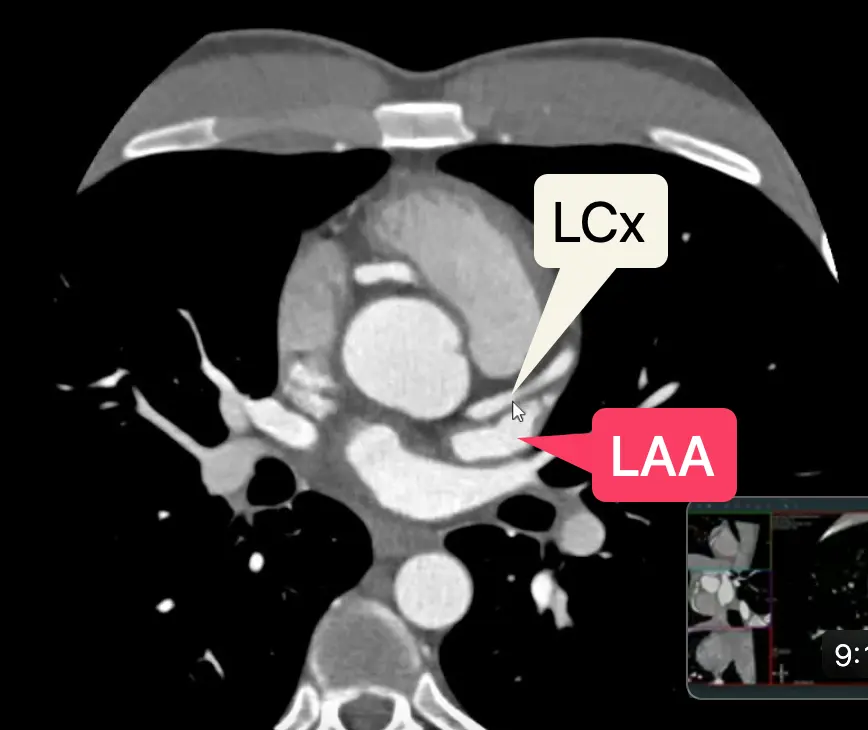
- LCx
- Reset your view and line up 2 orthogonal views → visualize SAX view
- By definition, the LCx travels within the L atrioventricular groove, which will course below the LAA.
- In some patients, you may see a small caliber “true” LCx (which you’ll know b/c it travels along the L AV groove) and a dominant OM, which appears large/beefier by comparison.
- You may appreciate the SA nodal branch, which arises off of the proximal LCx and extends to the atrial septum
’C’ view of RCA
Useful to view RCA and LCx
Both the RCA and LCx lie along the atrioventricular groove, so the ‘C’ view is useful to evaluate the RCA and LCx. When you get your RCA lined up (as below) in the MIP projection, you can scroll along and assess the LCx as well.
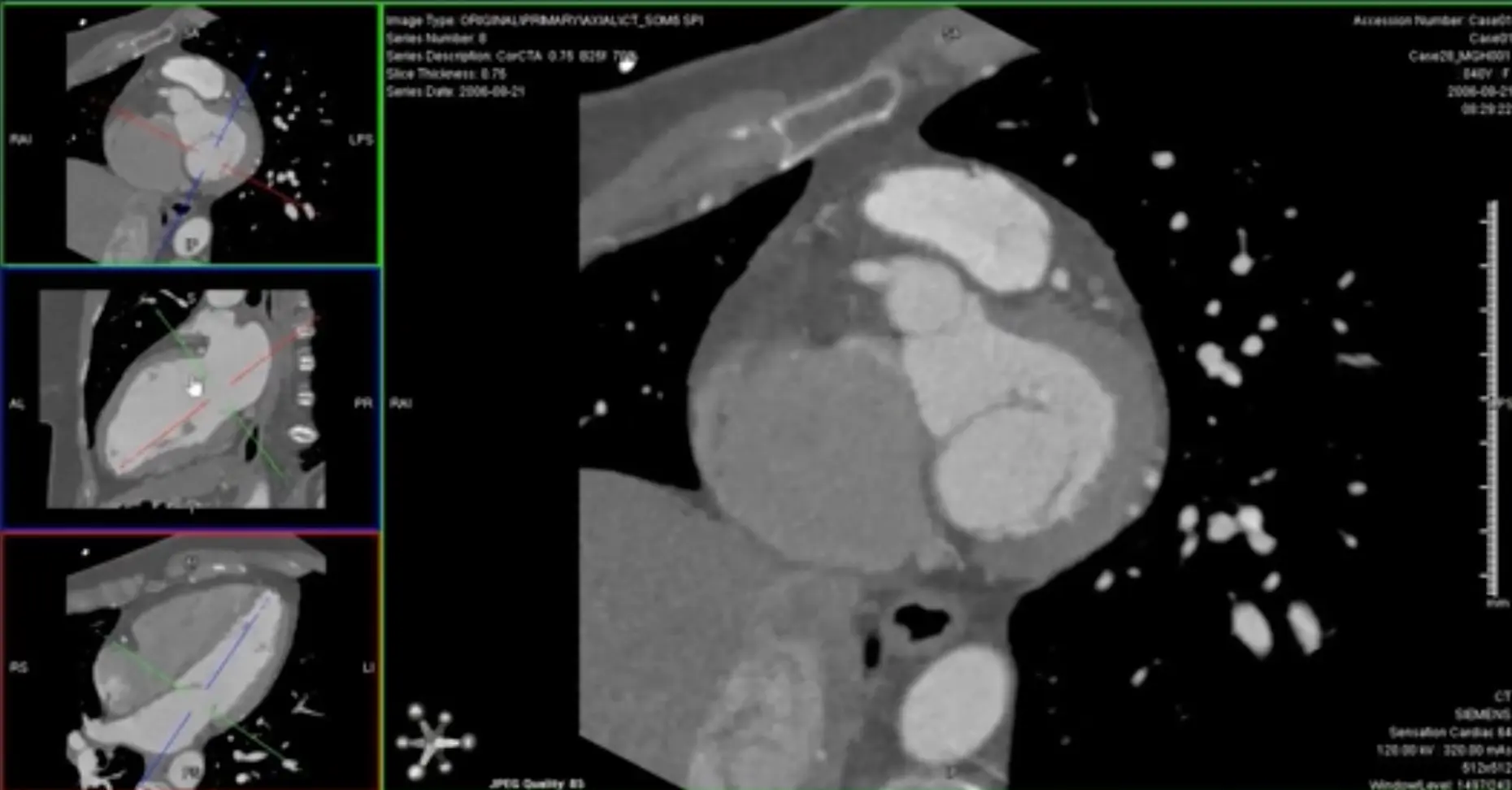
- Coronal view: Position crosshair (⌖) at mid-RCA
- Axial view: center on the SAX view of the RCA
- rotate ⌖ in the axial view until you are aligned parallel to the ventricular septum on your coronal window
- In your axial view, rotate ⌖ to align the orthogonal view (e.g. coronal window) so that the orthogonal view is along the atrioventricular groove
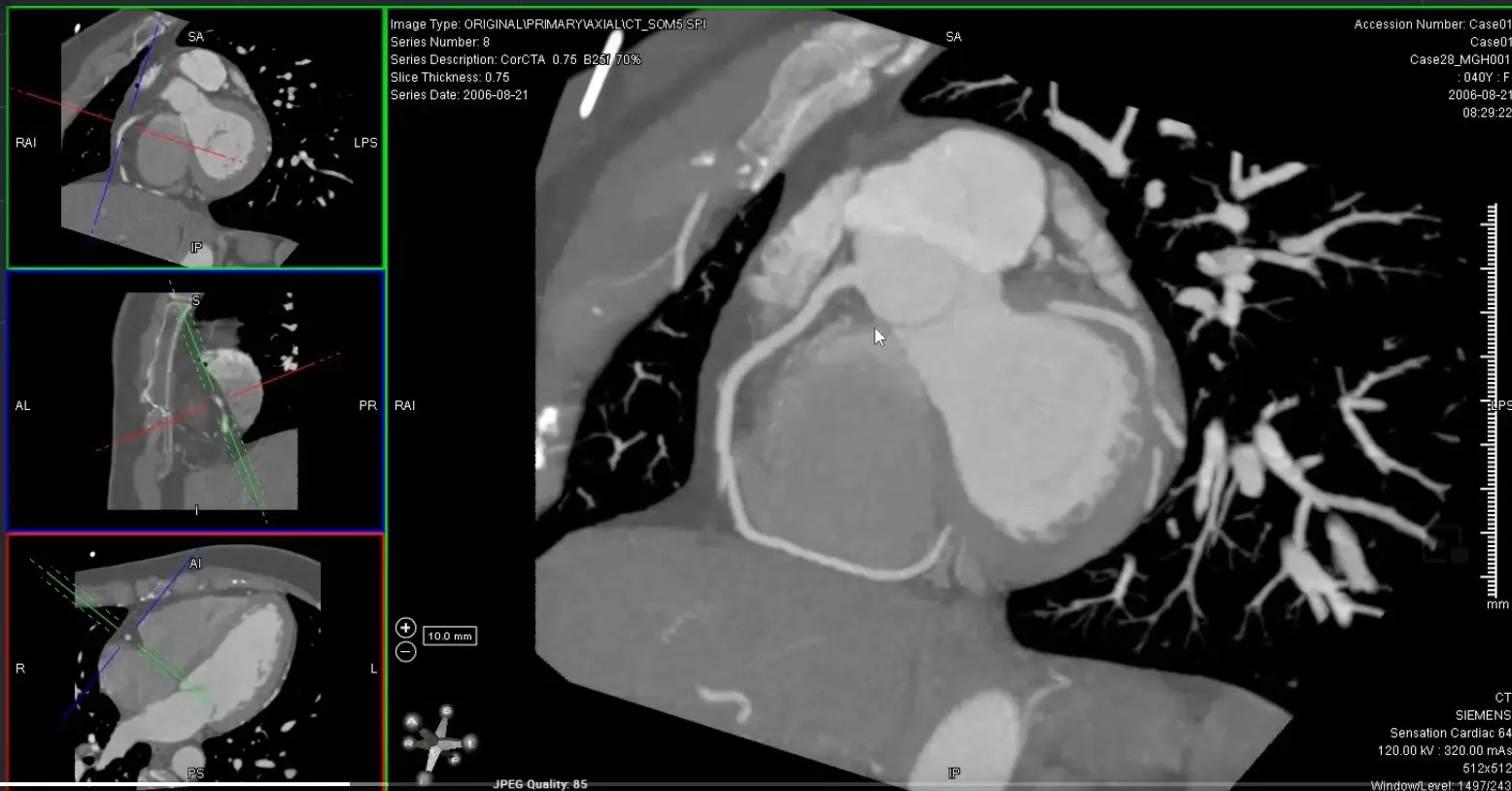
- Switch to MIP view
- MIP will help give you an overview of the vessel. Once you identify some areas of concern → switch to thin-slice images for closer investigation 🔍 and evaluation for stenosis.
- Go down to the thinnest possible section within the MIP view
Avoid assessing diameter stenosis using thick-slab MIP
When quantifying stenosis, you will always want to use thin slice images.
MPR of ‘C’ view of RCA
Above, but changed to MIP
Cardiac Chamber evaluation
Left Heart
- On axial view, line up the ⌖ so that it is centered at the level of the mitral valve and the line goes through the LV apex
- In the remaining window where the LV looks like it is in the 2-chamber view, also line up the ⌖ so that it is centered at the level of the mitral valve and the line goes through the LV apex
-
The remaining third window is now our short axis (SAX) view → scrolling through this window gives you the SAX orientation of the LV (similar to Cardiac MRI)
- Scroll through from apex → base (or base → apex, if you’d like) and examine the LV cavity, filling defects, structural abnormalities, integrity of the ventricular septum
-
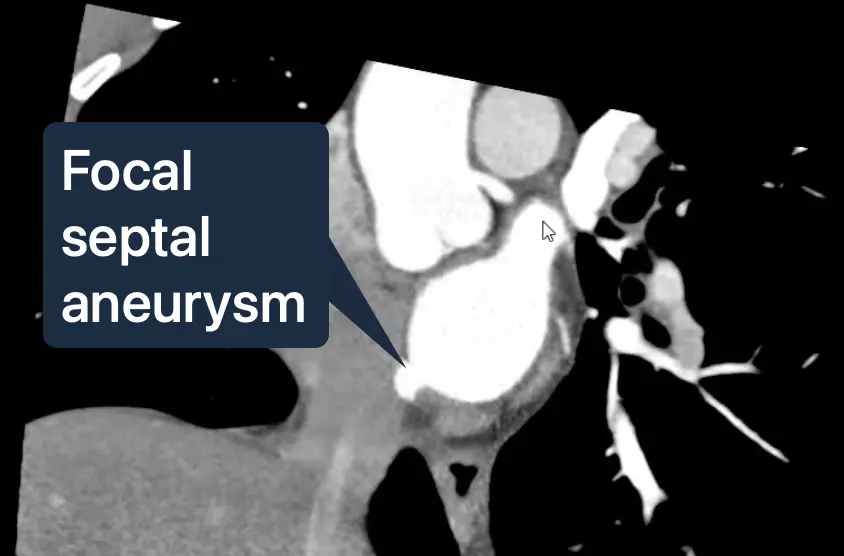
If you continue to scroll up, you’ll be at the level of the Left Atrium
-
You may see a focal atrial septal aneurysm between the LA and RA, which are often associated with small PFOs
-
Ischemia may appear as subendocardial hypoattenuation, fatty metaplasia or calcification
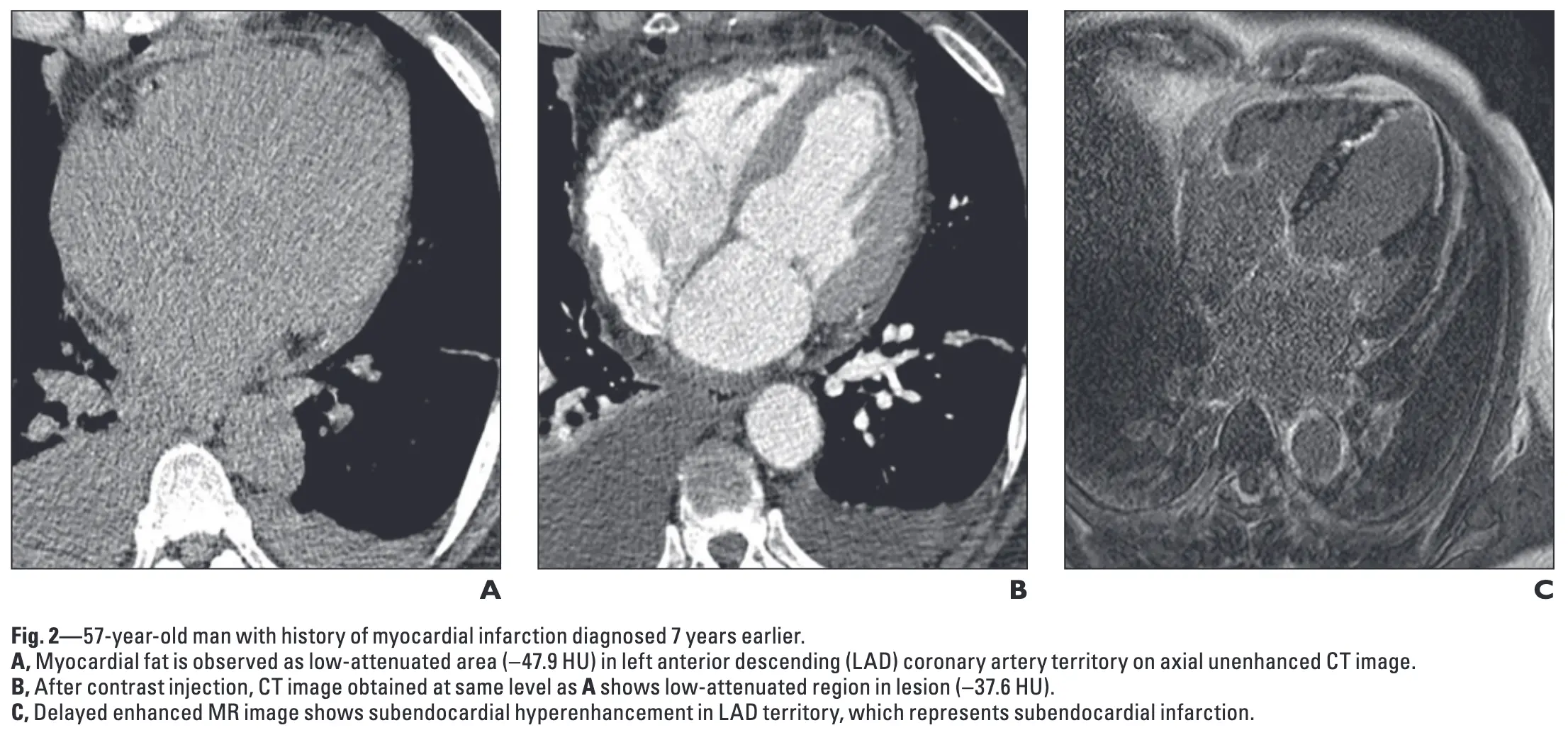
- Figure source: 1
Left Atrial Appendage
- Open your 2-chamber (2CH) view (aka vertical long axis/VLA)
- Also provides a different view to assess the MV leaflets
- Scroll through to assess for any filling defect
Right Heart
- Open your 4-chamber (4CH) view (aka horizontal long axis/HLA)
- The RV will have a prominent moderator band and relatively greater trabeculations (compared to the LV)
- The tricuspid valve may be difficult to closely evaluate
- When inspecting the RA, you may see a whisp of contrast entering from the LA with flow that is parallel in direction to the interatrial septum suggestive of PFO
- Scrolling further down
- Coronary sinus extending into the RA
- Inferior cavoatrial junction
- IVC
Pulmonary veins → Left Atrium
- While still in your 4-chamber (4CH) view (aka horizontal long axis/HLA), scroll up/down to assess the pulmonary veins to see that they are draining into the LA
Pericardial evaluation
- After resetting your images, use your axial images and scroll up/down
- Look for:
- pericardial thickening
- ≥1.5-2 mm on thin section images would be questionably abnormal
- pericardial calcification
- pericardial effusion
- pericardial thickening
Great Vessels
Ascending Aorta
- To create a short axis of the aortic root →
- Center your ⌖ at the level of the AV in 2 orthogonal views along the long axis of the aortic root

Pulmonary artery
- Reset, then in your axial view → find your main pulmonary artery and align the ⌖ at the center of the main PA. Get your SAX to make measurement by aligning 2 orthogonal views along the long axis of the main PA.
- In general, the main pulmonary artery should measure <2.9 cm in diameter.
Lungs
Mediastinum
Footnotes
-
Ahn SS, Kim YJ, Hur J, Lee HJ, Kim TH, Choe KO, Choi BW. CT detection of subendocardial fat in myocardial infarction. AJR Am J Roentgenol. 2009 Feb;192(2):532-7. doi: 10.2214/AJR.08.1608. PMID: 19155421. ↩