- Relatively common and generally carries little prognostic significance.1
- Most younger patients with RBBB have no underlying heart disease
- In fact, prognosis has little to do with the RBBB itself and more to do with the underlying process that causes the RBBB
- With a functional Left bundle, i.e. isolated RBBB, then these patients do not appear to suffer from clinically significant ventricular dyssynchrony → LV contractions remain coordinated and efficient.
- Incidence ↑ with age 1
- <1% in 50 yo → 10% in 80 yo
- Common in conditions that affect the right ventricle, e.g. Pulmonary Hypertension, right ventricular hypertrophy, RV inflammation or infarction. Can also appear abruptly with sudden ↑ in R-sided filling pressures, e.g. Pulmonary Embolism.
Masquerading Bundle Branch Block (MBBB)
- Suggested by presence of QRS morphology resembling RBBB conduction in the precordial leads but resembling LBBB conduction in the limb leads 2
- Special type of IVCD that although uncommon, is important to recognize because it identifies a group of patients with:
- Very severe underlying heart disease
- A much higher predisposition for developing complete AV block (and needing a pacemaker)
- An extremely poor long-term prognosis
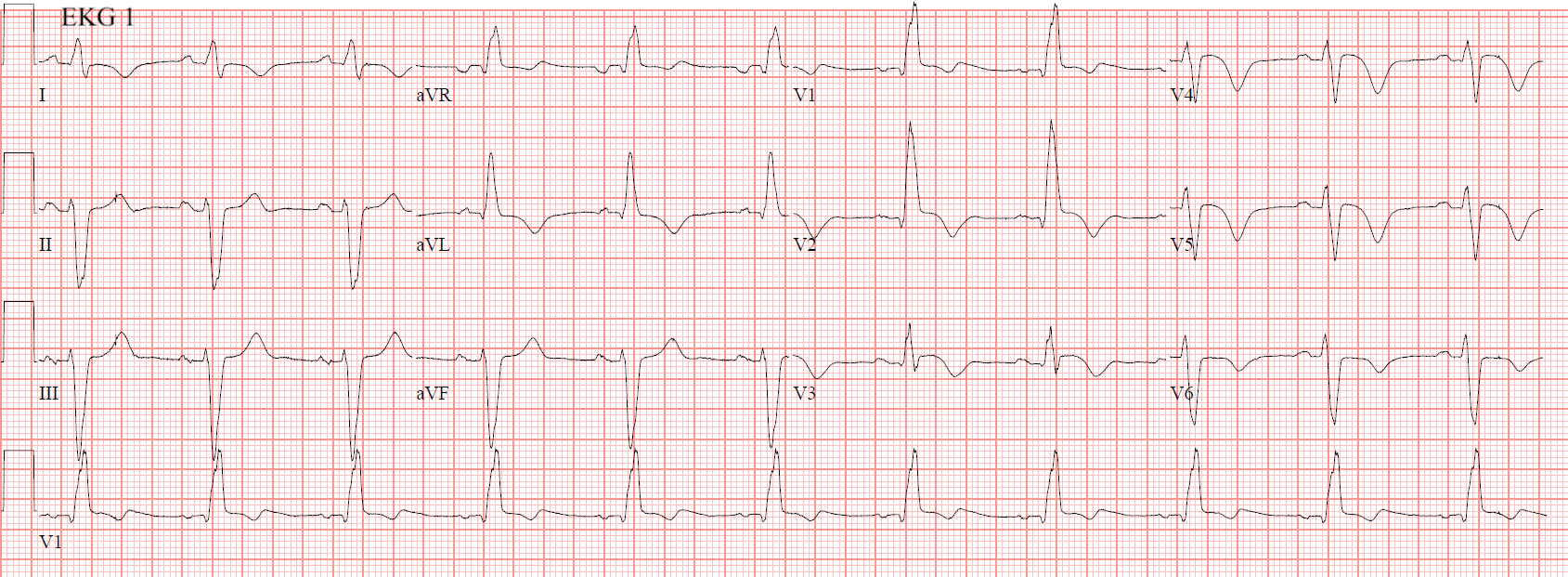
ECG Features
- Widened, R-R’ appearance detected in leads V1 and V2
- Most commonly will have a rsR’ appearance in V1 with (appropriate) discordant T wave changes, i.e. inverted T wave
- Most commonly will have a rsR’ appearance in V1 with (appropriate) discordant T wave changes, i.e. inverted T wave
- Wide, slurred S wave in lateral leads (I, aVL, V5-6)
- In RBBB, the ST segment should be depressed up to 1 mm in V1-V3, i.e. discordant to the R’-wave (or >1 mm in the case of a high voltage R’-wave, such as in RVH) 2
- ∴ ANY STE in V1-V3 in a patient with RBBB is OMI until proven otherwise

Footnotes
-
Fogoros, R. N., & Mandrola, J. M. (2017). Fogoros’ electrophysiologic testing. John Wiley & Sons. ↩ ↩2
-
https://hqmeded-ecg.blogspot.com/2025/04/never-send-chest-pain-patient-home.html ↩ ↩2