- On ECG, some P waves are followed by QRS complexes, and others are not.
- ==Symptoms are largely dependent on the ventricular rate.==
- The Mobitz classification helps to localize the site of the 2˚ AVB.[^fogoros]
- Autonomic maneuvers can be used to distinguish between AV nodal vs. distal/infranodal block if Type 1 or 2:1 AVB:
- If AV nodal block, exercise/atropine will improve/resolve the block
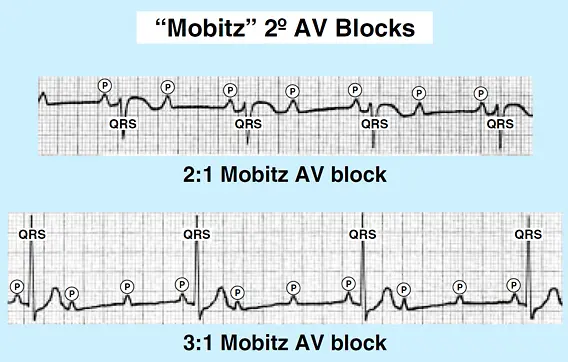
- If distal block, exercise/atropine will not improve the block and may actually worsen the block, e.g. 2:1 → 3:1 (or higher)
Cannot use Mobitz classification in 2:1 AV block
You cannot use the Mobitz classification with 2:1 AV block (by definition). Many clinicians make the mistake of automatically classifying 2:1 block as Mobitz Type 2, i.e. misdiagnose 2:1 AVB as distal block. When 2:1 block present, use another classification besides Mobitz to deduce the site of the block.[^fogoros]
Mobitz Type 1 (aka Wenckebach)
Detecting Mobitz Type 1 on ECG
The best way to tell that the Mobitz 1 pattern of PR prolongation is occurring is to compare the PR interval of the last conducted beat prior to the dropped beat with the PR interval of the first conducted beat after the dropped beat. In other words, compare the “longest” conducted PR interval to the “shortest” conducted PR interval.
- vagally mediated → ↑ in vagal tone leads to PR prolongation
- The site of block in Mobitz Type 1 is usually (but not always) localized to the AV node.
- PR interval gradually prolongs, then dropped QRS
- Treatment
- Typically none unless symptomatic
- Consider withdrawing AV nodal blockers (although typically not done)
Mobitz Type 2
- ==The site of Mobitz Type 2 block always indicates distal/infranodal block.==
- dropped QRS, but without the gradual prolonging of the PR interval
- can progress to Complete Heart Block (CHB)
- Cause: Conduction disease
- Treatment
- Pacemaker
- Consider temporary pacemaker until permanent pacemaker is implanted